
Our solutions
No search results
Wound care
(…) they affect up to half a million people in our country. If we add to this the number of family members caring for the people, that number will increase up to 1.5 million people directly related to the subject of chronic wound treatment (…)

The term “wounds” often evokes the notion of cut and stab wounds, which is a result of all sorts of crime fiction, novels and thrillers. These wounds of course require professional treatment and dressings but heal more quickly. It is much more difficult to treat so-called chronic wounds, which occur in up to half a million people in our country. If we add to this the number of family members caring for the people, that number will increase up to 1.5 million people directly related to the subject of chronic wound treatment, and thus – the principles of selection and dressing change.
Treatment of chronic wounds, or such as diabetic foot and pressure ulcers, and even burns, often lasts for months. It is very inconvenient for family members, as well as difficult for the person affected by this problem. This article is to encourage to become familiar with modern methods of chronic wound treatment in a moist environment, in accordance with principles developed by researchers. Let this article serve as an introduction to the topic and let it be some kind of hint, how in a modern way effectively and quickly treat chronic wounds.
Speaking of the modern chronic wound treatment, we do not recognise traditional dressings as bad. Traditional gauze dressings, bandages and plasters are good! No one questions their effectiveness, because they are perfect for the treatment of acute wounds (i.e. those resulting from mechanical reasons e.g. cuts, stab wounds, gunshot wounds and abrasions). In those cases sterile gauze dressings and plasters are most appropriate to be used.
EFFECTIVE CHRONIC WOUND TREATMENT
In case of chronic wounds (such as bedsores, burns, diabetic foot) as already as 40 years ago specialists discovered and clearly stated which conditions favour their rapid healing. This is the complete opposite to what traditional dressings provide. It turns out that a chronic wound will heal better if the following conditions are met:
- moist wound healing environment – promotes natural wound cleansing processes, regeneration of damaged tissues and reduces pain. This allows the wound to heal on average 50% faster;
- reduced pH value – lowering the pH value, the acidity of the wound environment increases, inhibiting bacterial growth;
- tightly closed wound (occlusion) – protects the wound from being infected by bacteria present in the patient’s environment. The use of special dressings of polyurethane foams also protects the wound against mechanical damage;
- stable temperature – stable temperature of about 37°C accelerates cell division, and thus regeneration of damaged tissues.
 FEATURES OF A PERFECT DRESSING
FEATURES OF A PERFECT DRESSING
Continuing research conducted by Georg Winter since 1962, William Tuner collected and summarised their results and presented them in 1979, defining the qualities of a perfect dressing. According to W. Turner a dressing, which, according to the modern (wet) wound healing model, will facilitate the healing process should:
- maintain optimum moisture in the wound,
- remove excess exudate and toxic components,
- isolate the wound thermally,
- allow gas exchange between the wound and the environment,
- be impermeable to bacteria and other microorganisms,
- be free from toxic particles and substances,
- provide protection for the newly formed tissues,
- be easily removed from the wound surface, without causing injury.
Dressings meeting the above criteria form a moist environment that favours important processes which take place in the wound, so that the healing process is about 50% faster with reduced sensation of pain and reduced risk of infection.
Why, despite the presence of a whole range of advanced dressings, the choice of the right one is so difficult?
Good identification of processes appearing during the wound healing process resulted in creating many specialised dressings with a number of very different characteristic features. Paradoxically, a large variety of dressings raises dilemmas about accurate selection in a specific situation. Remember that the decision to use a given dressing determines its effectiveness or lack thereof.
HOW TO CHOOSE THE DRESSING TO THE WOUND?
It seems that the choice of dressing must meet two basic criteria – we must remember that according to the modern wound healing approach there is no universal dressing that would meet requirements of every wound, and that choice must be aware, based on the correct diagnosis of the processes taking place in the wound and suitable for that characteristic features of the dressing.
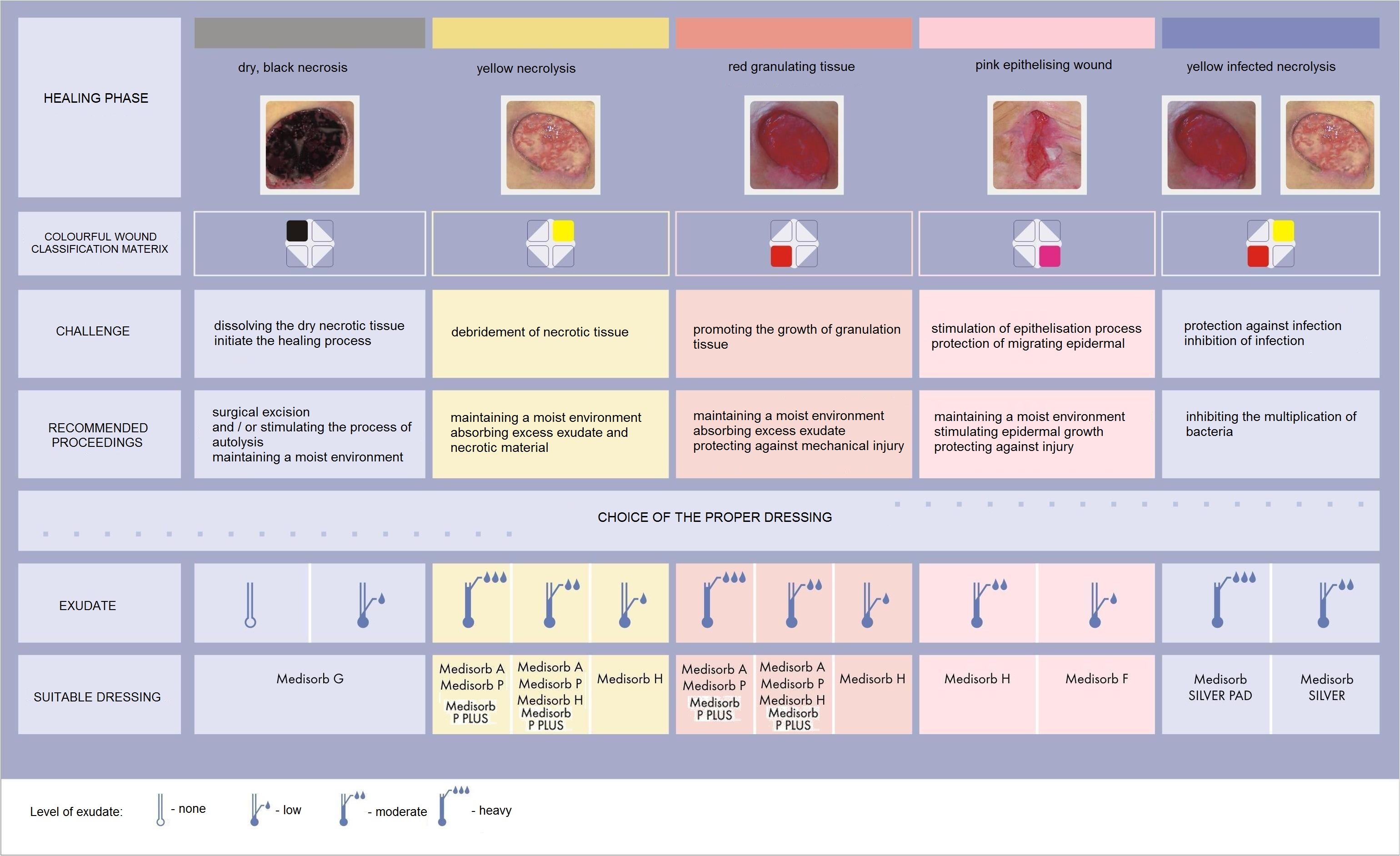
To facilitate the correct dressing choice, you can use the wound classification based on the phenomena that take place in different phases of wound healing and based on that wound colour assessment.
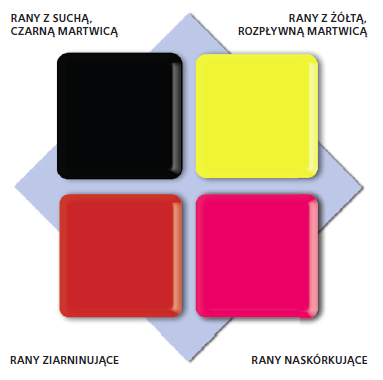
The scale consists of four colours respectively assigned to the specific stages of the wound healing process.
Selection of the dressing to the given wound while using the wound colour classification system becomes easier, because the wounds of the same type (colour) set similar challenges, and therefore require a similar procedure.
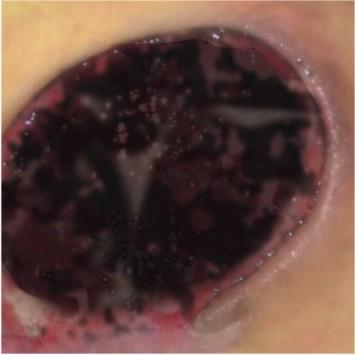
„BLACK” WOUND – NECROTIC TISSUE

OBJECTIVE OF THE TREATMENT:
- removal of necrotic tissue
WOUND CHARACTERISTICS:
- in form of dehydrated dead tissue
- necrotic tissue covers the entire wound or is present locally in form of patches
- exudate level – low (up to the point where necrosis turn into liquid discharge and separates from healthy tissue)
- necrotic tissue inhibits the healing process – it is the source of infection for healthy tissues, constitutes a barrier to the building new tissue
PROCEDURE:
- it is necessary to remove necrotic scab by a surgeon or in the autolysis process by the maintenance of a moist environment
RECOMMENDED DRESSINGS:
„YELLOW” WOUND – NECROLYSIS


OBJECTIVE OF THE TREATMENT:
- removal of necrotic tissue and preparing the wound bed for granulation
WOUND CHARACTERISTICS:
- cream colour of the wound – yellow, fibrous
- exudate level: high, medium, rarely low
PROCEDURE:
- maintain a moist wound environment
- control the level of exudate
RECOMMENDED DRESSINGS:
- Medisorb SILVER and SILVER PAD – infected wounds with high level of exudate
- Medisorb A – deep wounds with high or medium level of exudate
- Medisorb P – shallower wounds with medium level of exudate
- Medisorb P PLUS – shallower wounds with quite high level of exudate
- Medisorb H – moderate and low exuding wounds
- Medisorb G – infected wounds with low level of exudate (promotes wound cleansing by binding pre-hydrated dead tissue with microorganisms that colonise it)
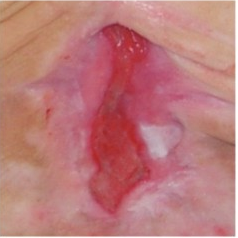
„RED” WOUND – GRANULATING TISSUE


OBJECTIVE OF THE TREATMENT:
- maintain a moist wound environment conducive to granulation
- control the level of exudate
WOUND CHARACTERISTICS:
- wound in a bright red colour, moist
- uneven wound surface
- the tissue is delicate, sensitive to pain, susceptible to infection
RECOMMENDED DRESSINGS:
- Medisorb A, Medisorb P or Medisorb P PLUS – heavy and moderate exuding wounds
- Medisorb H – moderate and low exuding wounds
- Medisorb G – infected wounds with low level of exudate (promotes wound cleansing by binding pre-hydrated dead tissue with microorganisms that colonise it)
- Medisorb A – in case of infected wounds with high level of exudate
„PINK” WOUND – EPITHELISING TISSUE

OBJECTIVE OF THE TREATMENT:
- protection of new tissue
- stimulation of skin formation
WOUND CHARACTERISTICS:
- pink or white tissue appears on the wound surface
- epithelial cells migrate from the wound edges to the centre
PROCEDURE:
- encourage or support the process of skin formation
- maintain a moist wound environment
- protect against mechanical damage
RECOMMENDED DRESSINGS:
- Medisorb H – moderate exuding wounds
- Medisorb F – low exuding wounds
Anna Rogalewska, Patrycja Judycka
Toruńskie Zakłady Materiałów Opatrunkowych SA
Evolving trends in wound dressing
From herbs and leaves, to gauze and bandage, to professional dressings, the practice of wound dressing has been evolving for tens of thousands of years. For over 60 years, Toruńskie Zakłady Materiałów Opatrunkowych (TZMO) has been delivering trend-setting products in wound dressing. Over the years, we have made changes to our range of dressings and the way we make them, but one thing has been constant: we continue to take care to deliver top-quality products that meet the most rigorous safety standards. TZMO’s Matopat-branded medical products have always been a symbol of high quality, innovation and biocompatibility.
Choosing the right dressing: What should patients take into account?
First of all, it’s the kind of wound, as different wounds heal differently. You will need a different dressing for a surgical wound, or incision (such wounds must be dressed precisely, in a sterile manner, by qualified medical personnel in a suitable place), a different one for a new post-injury wound and a yet different one for a difficult-to-heal wound with substantial tissue loss. Once you have identified the kind of wound you’re dealing with, you need a professional dressing that will not only reduce the risk of infection and offer optimal healing time and effectiveness, but also help the patient feel more comfortable. There has been a noticeable trend in the use of professional wound dressings: in the past, they were used only by medical professionals in hospitals, but now they are making their way to pharmacies. As a result, professional wound dressings can today be used by patients at home.
The properties of professional wound dressings
For a small cut or chafe, a clean and comfortable sticking plaster will do the job. Apply it to the affected area and leave it for a scab to form and the wound to heal. However, in the case of more serious wounds, such as surgical wounds, it is advisable to use professional dressings such as those used in hospitals. Professional surgical dressings are sterile, absorptive and flexible, and designed so that the adhesive can keep the dressing tight on the affected area, preventing dirt or other unwanted matter from penetrating the wound. At the same time, the absorption material should be sufficiently protected to prevent direct contact of the dressing with the surface of the wound or with the surgical sutures. Professional dressings are also air-permeable to allow the skin to “breathe”.
 Examples of professional dressings for surgical wounds include Fixopore S and Fixopore F. The former is made of flexible, nonwoven fabric that easily fits in even hard-to-access areas of the patient’s body and will not limit the patient’s movement. A nonwoven fabric dressing is the basic type of dressing used by hospitals for surgical wounds. This dressing has a special, smooth layer of absorption material that will not get stuck on the wound or suture, thus allowing for safe and painless dressing changes without the risk of damage to the absorption material. The adhesive on the dressing is hypoallergenic. The other of the two products, Fixopore F, is made of ultra-thin polyurethane film that keeps moisture away from the wound. This helps patients to go about their regular daily activities without having to change their dressings frequently and without the risk of infecting the wound. The benefits of modern wound dressings can be enjoyed fully if the dressings are used in accordance with the user’s instructions.
Examples of professional dressings for surgical wounds include Fixopore S and Fixopore F. The former is made of flexible, nonwoven fabric that easily fits in even hard-to-access areas of the patient’s body and will not limit the patient’s movement. A nonwoven fabric dressing is the basic type of dressing used by hospitals for surgical wounds. This dressing has a special, smooth layer of absorption material that will not get stuck on the wound or suture, thus allowing for safe and painless dressing changes without the risk of damage to the absorption material. The adhesive on the dressing is hypoallergenic. The other of the two products, Fixopore F, is made of ultra-thin polyurethane film that keeps moisture away from the wound. This helps patients to go about their regular daily activities without having to change their dressings frequently and without the risk of infecting the wound. The benefits of modern wound dressings can be enjoyed fully if the dressings are used in accordance with the user’s instructions.
Educating patients
A pharmacist’s role is not only to help patients choose the right dressing, but also to educate them about the need for taking proper care of their wounds. Wound cleaning and correct dressing changes are essential and, apart from the choice of dressing, will help the wound to heal quickly and without complications. A general rule in professional wound healing is that dressing changes should be as rare as possible, following the recommended dressing use time, and as frequent as possible, depending on the appearance of the wound and the condition of the dressing.
For more information about professional dressings for different wound types, please visit: en.matopat-global.com
Yearly about 1% of our population gets burned. The number of Poles affected by burn injuries reaches even 400,000 patients a year. Mostly 50-80% of the burned are children in the 2-4-year-old age group.
Burns can be divided by depth:

- 1st degree – a superficial burn. Only the surface layers of the skin are affected. The symptoms include redness (erythema) and painfulness. The wound usually heals without any complications and scars.
- 2nd A degree – extends into superficial (papillary) dermis. Those wounds are usually very red with clear blisters and are extremely painful. After 2nd A injuries there might appear small discolorations or even scars.
- 2nd B degree – extends into deep (reticular) dermis. In those type of burns superficial epidermal and dermal necrosis might appear. Those wounds are very painful, without blisters, pale or pinkish, grey, bricky or even black. Moreover, they may leave nasty hypertrophied scars.
- 3rd degree – extends through entire dermis. These wounds are usually russet, brown, pale yellow or red.
- 4th degree – extends through skin, subcutaneous tissue and into underlying muscles, tendons, bones, joints.
In the 3rd and 4th degree burns the skin reproductive layer is impaired or completely damaged.
Complications of burns
Quite a frequent complication of burns are hypertrophied scars and joint contractures. The hypertrophied scars appear, among other things, as a result of the increase in blood flow, fibroblast development and collagen deposition as well as of chronic oedema. In all those cases, when strong redness of the scar does not disappear up to two months, and the scar gets thicker and thicker, a keloid scar is very likely to develop. Keloids have a lumpy structure, which is a result of increased metabolism. Their growth is stimulated by microphages and fibroblasts, evoking an overgrowth of collagen fibres. Those complications are inconvenient because they delimit the functioning of the motor apparatus and at the same time they blemish the affected person.
Prophylactically appropriate positioning of the body and joint immobilisation by means of splints or orthopaedic devices is practised. It has also been proven that the application of constant pressure, increasing the capillary pressure of vessels i.e. about 25-30 mmHg, has a beneficial influence on scar formation, and prevents the overgrowth to a large extent. A long-lasting pressure causes an oxygen deficiency in tissues, a deceleration in metabolism and a fibroblast reduction. An increase in the activity of a collagen-decomposing enzyme (collagenase) results in a visible scar reduction.
The pressure method in supporting the post-burn scar treatment has been worldwide known for many years, and it is also commonly used in Poland. The pressotherapy is found to be the most effective method, though there are many alternative ones such as laser therapy, kriotherapy etc.
Apart from negative health effects, quite often the keloids are also harmful to patients’ mental state, resulting sometimes in social exclusion. In modern techniques, and medical procedures it is clearly stated that an effective post-burn rehabilitation needs to be designed in such a way to reduce the keloid formation. An important element of modern treatment support techniques is the application of compression combined with the activity of silicone dressings like e.g. CodosilTM ADHESIVE.
Mechanism of post-burn scar formation
Every wound has the possibility of self-healing. Superficial wounds, in which the topmost layer of the skin (the epidermis) is scraped off, heal without leaving any scars. At the beginning of the healing process the wound is cleansed, so there appear a lot of macrophages and histiocytes. The neoformation of capillaries is evoked, facilitating the appearance of multipotent cells – lymphocytes, which have the ability to turn into fibroblasts. A fibroblast is a type of a cell that synthesises the macromolecules building connective tissue. This cell synthesises tropocollagen, which by polymerisation creates collagen fibres. As those fibres get created, the involution of capillaries takes place, the activity of fibroblasts is lost, and the reepithalisation process is initiated.
In burns, when the epidermis, the papillary layer and the reticular layer get damaged, a stronger hyperplasia of vessels is observed. The widening of vessels, and the appearance of anastomoses causes blood to stop in the healing place, and provides a good access to nutrients; a lot of highly active fibroblasts appear as a result of the production of a great number of collagen fibres.
The reconstruction along with the scar formation takes place at the newly created fibroblasts’ expense, where gradually myofibroblasts – responsible for contractility – get distinguished, while mastocytes take care of the progressive maturation of the scar. Biochemical tests of a scarring process show that there is an increased collagen synthesis in comparison with a normal healing process, and there are also qualitative disorders connected with the increase in the number of mucopolysaccharide matrices, and the decrease in the number of lipids (mainly linolic acid) in the scar. It seems that the reason for this lies in the reduced amount of collagenase (a collagen-decomposing enzyme), resulting from the increase of 1 – antitrypsin and 2 – mucoprotein globulins. Those effects occur probably along with a toxic mitochondrial activity in the damaged cells. This activity takes place in burns from the first moment up to the 10th day of the healing process, when it is possible to notice that those symptoms stop, and a gradual comeback to a normal state, or also an objective steady growth takes place up to the 14th and after the 21st day, if any scarring complications appear.
Moreover, also the effect of the adrenal gland on scar fibroblasts, and their uncontested influence on scarring processes has been recognised. This is the base to examine possible mutual correlations between the prevalence of scarring complications and endocrinological changes in children. Obviously such a correlation takes place during a burn shock, and its further development is not known. Topical scar complications developing after a burn can be either of an aesthetic or of a functional type, or of both types simultaneously. From a histopathological point of view the cicatrical changes are of a hypertrophic, a contractile or a keloid type. Popularly it is said that this happens in 50% of burn cases; however, the factors indicating those changes has not been determined yet. Their impact on the early estimation of an actual scar development possibility is also not known. Especially when it goes about keloids – they are likely to develop even in 80% of places vulnerable to stretching or tension.
Pressotherapy – an effective therapeutic method for post-burn scars
An elastic pressotherapy as a preventive and therapeutic method started to evaluate in the 70s, and turned out to be very effective in supporting the treatment of post-burn complications. This method involves using hypercompression (or just compression) to give constant pressure on keloids. This pressure on the scar gives an ischemic effect, which makes afferent vessels smaller, which results in the reduction of vessel embryos. On one hand, the scar will be supplied with less blood if we reduce the number of blood vessels, but on the other hand, depending on the diameter of the vessel embryos, the blood flow will be increased, and there will be no stasis, which will further influence the reduction of produced collagen fibres, and prevent the wound area from shrinking.
A correctly applied pressotherapy involves the use of strong pressure on the wound after finished epithelisation by means of different types of bandages made of natural latex. Such products are produced of latex threads covered with synthetic fibres.
Their application on the scar and the stable pressure they give can change and improve the content and the quality of various tissue elements. This change in the tissue components results in the qualitative improvement, weakening and decreasing the size of the scar, and at the same time due to the accompanying ischemia, the characteristic red colour of the scar is fading.
General rules for the use of pressotherapy:
- the pressure should be applied as soon as possible (from the moment of wound re-epithelisation, during the next 2-3 years – this is the estimated time for scar development), more or less 1 or 1,5 year;
- constant uninterrupted and long-lasting application of pressure on cicatrical places through an individual adjustment of special compression garments with compression level from 20-25 up to 50 mm Hg/cm2.
To reach the best results it is necessary to observe and control the entire process of the compression rehabilitation, and to change the compression garment periodically since the knitted fabric loses its elasticity, or the patient’s size might change as well.
The time of the compression therapy is varied – optimally up to 2 years. If any topical complications appear such as skin irritation, intertrigo, skin breaks or patient’s psychical inconvenience – the pressotherapy should be temporarily interrupted and then repeated, trying to eliminate those symptoms. [1]
Compression levels in pressotherapy
Compression clothing is characterised by a precisely defined pressure level exerted on the patient’s body. The pressure is expressed in a unit – millimetre of mercury (mmHg). The efficiency depends on the size of the garment, which is to be individually adjusted to a given person after taking precise measures of the patient’s body. The effectiveness of the therapy is also affected by the choice of an appropriate compression level, which depends on the disorder type and its severity. It is highly important to choose the right compression level of a compression product, for too little pressure will bring no effect, and too big pressure can cause many undesirable side effects. The complications may start from very simple ones such as chafes, abrasions or maceration, up to more serious ones such as serous blisters or decubitus ulcers. Those and other side effects resulting from a wrongly chosen compression level, quite often make the patient break the therapy.
The most popularly used compression level classification is the one used in Germany, Switzerland and Italy. In all types of classifications class 1 means the lightest compression, and class 4 the strongest compression. The values express compression given by a product at the ankle joint high. It is important to maintain a compression gradation given on the limb at the entire length of the product. In this case usually there is a rule applied to use 100% compression of the given class (from 1 to 4) at the ankle high (distal part of the product), up to 40% of the compression in the closer (proximal) part.
Producers use different classifications of compression; however, the one specified by the European Standardisation Commission distinguishes the following ones:
- class 1 – light compression (18-21 mmHg),
- class 2 – medium compression (23-32 mmHg),
- class 3 – strong compression (34-46 mmHg),
- class 4 – very strong compression (over 49 mmHg).
Efficient therapy with the application of compression garments Codopress®
The success of the therapy highly depends on appropriately chosen compression clothing. Compression garments Codopress® produced in Łódź (Poland) by Tricomed SA are used for supporting the treatment of post-burn scars and in prophylactic rehabilitation of burns. Up till now over 20 thousand products Codopress® have been prepared, successively developing the product range, and improving the construction. The garment is produced of a highly elastic breathable knitted fabric of medical quality, composed of a polyurethane and polyamide yarn. This combination enables to obtain required parameters, and at the same time to provide high comfort for the user.
The manufacturing process makes it possible to produce the garment for every body part according to the compression class recommended by a doctor. The 1st class compression (18-21 mmHg) is the one most frequently used. It is remarkable that all compression products Codopress® are manufactured so that all seams are aside from all scars. Thanks to this the value of the therapeutic pressure is not changed in any way in this place.
The process of compression garment preparation:
- Get a referral from a specialist.
- Make an appointment with a person taking measures of the limb or other body parts.
- Once the garment is sewn it needs to be tried on to make sure that it fits perfectly.
- The patient is trained how to use and clean the product.
All compression garments should be worn permanently from 6 to 24 months after the wound healing process is finished, till visible rehabilitation effects appear (flattening, fading and softening). The entire therapy usually requires a few changes of the compression garments, along with the use up of the garment and the change of patient’s body size. It is important to remember to use the products only when the post-burn wound is fully healed – see pictures below:


Individually prepared Codopress® products:
- give appropriate compression on the scar,
- can be used with other types of therapy,
- cause no allergic reactions or skin irritations,
- release itching,
- prevent from joint contractures.
Clinical trials
In specialised burn healing centres in Siemianowice (Poland) and Polanica Zdrój (Poland) – leading centres healing heavy burns – a wide range of patients were clinically examined. They tested the effectiveness of Codopress® products in the rehabilitation of post-scar burns.
Clinics testing the Codopress® clothing included the Burn Treatment Ward of the Municipal Hospital No. 2 in Siemianowice Śląskie ran by S. Sakiel, MD, and the Plastic Surgery Hospital in Polanica Zdrój under the supervision of K. Kobus, PhD, Dr h. c. What is more in the National Medicines Institute under the direction of W. Zalewski, PD tests were carried out as for the irritating effect on the skin of the knitted textile used in the production of Codopress® products.
Materials and methods
Within 2 years compression products produced by Tricomed SA were tested in 40 patients at the age of 2 to 59 years old with the average burn area of 26%, and deep burns at the entire skin depth with the average area of 9%.
The patients were divided into two groups:
- in the first group (20 patients) the compression products were applied right after the wound was healed,
- in the second group (20 patients) the Codopress® products were applied after about 3 months after the wound was healed.
The evaluation concerned the face, the neck, the chest, the upper and lower limbs. Overall in the first group 24 places and in the second group 30 places were observed.
 The tested products were evaluated as for their usefulness in supporting the treatment of hypertrophied scars and keloids in 26 patients aged 3 to 58 years. Most of the hypertrophied scars and keloids were caused by hot fluids or fire. The entire healing period for a burn wound, starting from the application of the compression products, took a month up to 4 years. Before the application of pressotherapy, massages were applied. Body parts that were most often tested as for the usefulness of the compression products included: the knee and elbow joint, the buttocks, the hips, the shoulders, the chest, the upper and lower limbs.
The tested products were evaluated as for their usefulness in supporting the treatment of hypertrophied scars and keloids in 26 patients aged 3 to 58 years. Most of the hypertrophied scars and keloids were caused by hot fluids or fire. The entire healing period for a burn wound, starting from the application of the compression products, took a month up to 4 years. Before the application of pressotherapy, massages were applied. Body parts that were most often tested as for the usefulness of the compression products included: the knee and elbow joint, the buttocks, the hips, the shoulders, the chest, the upper and lower limbs.
Test results
The results of the carried out tests indicated that in hypertrophied scars and keloids treated with the compression products sweeping changes were noticed. The itch observed in 8 cases retreated after 3 weeks. The colour of fresh scars changed from bloody pale into flesh-like in 17 patients after 4 weeks. The height of the scar was reduced from average 4 mm at the beginning (measured from the healthy skin) up to 0-2 mm. The best results were observed in fresh scars, which were 4 weeks old. In the case of older scars those effects were visible after a longer period of time.
There were no allergic reactions noted. Washing by means of commonly available washing agents and an all-day-long utilisation did not affect the elasticity of the tested products. The best therapeutic results were observed on tights, lower legs and forearms. The patients had no objection to wearing the compression garments. All in all compression products Codopress® undoubtedly contribute to faster rehabilitation of patients with after-burn deformations.
The summary of test results
While wearing Codopress® products for a few months the following conclusions were made:
- the scars were getting flatter,
- the extremely red colour was gradually fading,
- no allergic reactions to the material in Codopress® products were observed,
- in the same patients comparing not pressed scar places with the ones pressed by means of Codopress® clothing there were visible differences in form of hypertrophies and hard scars in the not pressed places,
- the application of the compression clothing just after the wound was healed brought better effects than in patients who used the products after hypertrophied scars appeared. [2]

Conclusions
- The tested products Codopress® are very useful in the prophylaxis and rehabilitation of hypertrophied scars.
- Compression garments need to be tailored according to the measured body dimensions of the wearer in order to provide high efficiency.
- An early application (just after the wound is healed) of tailor-made compression products guarantees the best efficiency of the scar rehabilitation.
- Constant wear of the clothing (13 hours a day) 1 to 2 years changed only if it is worn up or the patient’s size has changed:
- prevents the development of hypertrophied scars,
- causes the reduction and, in most cases, the regression of keloids,
- improves the final aesthetic look.
- Pressotherapy enables to continue physical rehabilitation and does not constrain the patient’s activity after the burn.
- The knitted fabric used in Codopress® products causes no irritating reactions.
[separator]
Associable therapy Codopress® + Codosil™ ADHESIVE
Silicone dressings adjunctive to scar treatment by means of pressotherapy have gained in popularity in the past 10 years. Their application decreases the growth of small blood vessels in a scar, and as a result the scar gets more elastic and flatter.

Many specialists recommend the associable therapy, combining a few methods individually adjusted to a given patient. One of them is compression therapy joined with dressings meant for scar rehabiitation. The dressing used for this type of combined therapy is CodosilTM ADHESIVE.
CodosilTM ADHESIVE is a soft multi-layer product designed for the rehabilitation of hypertrophied scars and keloids. Adhesive silicone layer is in the direct contact with the scar surface. The outer side of the dressing is secured with an anti-adhesive protection layer.
- releases the itching and pain,
- does not present irritating and sensitising properties,
- is susceptible to folding,
- reveals sticky properties which makes it possible to stick to the skin’s surface repeatedly,
- is meant for multiple use,
- is easy to store and apply.
 The silicone dressing can be applied as a preventive agent when the wound is fully closed (8-10th day) or when first symptoms of a hypertrophied scar appear. Early application of the dressing increases the chance of proper scar rehabilitation.
The silicone dressing can be applied as a preventive agent when the wound is fully closed (8-10th day) or when first symptoms of a hypertrophied scar appear. Early application of the dressing increases the chance of proper scar rehabilitation.
The dressing is used only on skin that is not broken, remembering to make the dressing 1 cm bigger than the scar size. Prophylactically it should be worn 12 hours a day. In patients using the compression products Codopress® along with the silicone dressing CodosilTM ADHESIVE there were visible therapeutic effects observed: flattening, fading and softening of the scar. Moreover, the motor activity is improved and the risk of contractures is limited.
CodosilTM ADHESIVE is recommended to be used:
- in rehabilitation of hypertrophied scars and keloids,
- as prophylaxis in people with hypertrophied scar and keloid tendencies,
- in cosmetology for the rehabilitation of scars after aesthetic surgery.
Literature:
[1] Babiana Mossakowska, PhD, Professor, Presoterapia u dzieci (Pressotherapy in children).
[2] A. Nawrocki, doc., PhD, and others, Ocena kliniczna – Opracowanie technologii i ocena artykułów medycznych do zastosowania w chirurgii plastycznej (Clinical evaluation – The compilation of technologies and the evaluation of medical products to be applied in plastic surgery).
All Codopress® products are individually prepared after taking measures. To make an appointment and get more information please contact us export@tzmo.com.pl.
Elżbieta Szwałkiewicz
National Consultant in Nursing Chronically Ill and Disabled People
One of the indicators used to assess the quality of long-term care of an immobilised person is the skin condition in areas exposed to constant pressure. It would seem that nurses know everything on the prevention of pressure ulcers, and that is why I wonder what is the reason for such a high incidence of pressure ulcers in people who are under constant nursing supervision.

The scale of the problem entitles me to claim that in our country we have common and very serious failings in the care of the sick and disabled, both in stationary health-care and social assistance, as well as in home conditions. These neglects are the cause of immense suffering and generate substantial costs of treatment and care.
There have been many publications on the subject of pressure ulcers referring to numerous medical research and statistics. They repeat the same key information:
- the major etiological factor is the pressure on tissue located over bone prominences, leading to the development of necrosis and then to ulceration,
- skin damage occurs as a result of repeated pressure exceeds the average pressure in skin capillaries (32 mmHg), the impairment of sensation is a contributing factor,
- the formation of pressure ulcers is accelerated by skin maceration, which is a consequence of increased humidity due to urine and faecal incontinence or perspiration,
- the most common location is around the sacrum, ischiadic tubers, trochaners, ankles and heels,
- each immobilised patient is at risk of pressure ulcer formation,
- modern technologies ought to be used to reduce the pressure on the skin, such as specially designed mattresses, pillows, textiles and equipment for sliding movement, modern protective and therapeutic dressings, and aids absorbing urine,
- the treatment cannot be focused on the topical management of decubitus ulcer.
Basic principles relating to prevention:
- proper nutrition – adequate intake of protein, calories and fluids will prevent the occurrence of negative nitrogen balance, weakness and dehydration,
- reduction or elimination of pressure and friction on the skin – this effect is achieved through the use of pressure relief mattresses and pillows, frequent change of body position, application of proper rules for lifting and moving patients,
- strictly comply with the basic care principles of people with incontinence (also the faecal type), including:
- daily washing and cleaning after every contamination with excretions,
- systematic control of skin condition in areas exposed to moisture,
- using absorbent products adequate to the level of micturition,
- preventing skin inflammation through the use of special protective dressings,
- protecting the skin against overdrying and irritants (urine and sweat) through the use of appropriate skin care products.
Modern approach to the treatment of pressure ulcers and other chronic wounds favours wound healing in a humid environment with the use of various specialist dressings, which are applied depending on the type and the location of the wound.
Scientific studies and practical experience have shown that increased moisture in the wound stimulates epidermisation, and this, in turn, stimulates the growth of connective tissue underlying the skin. Specialist dressings compared to conventional gauze dressings also affect the rate of healing. They prevent the damage to the young epidermis during each dressing change, and they contain substances that affect the treatment and healing of wounds. Not to be underestimated is the fact that effective protection of the interior of the wound against external factors, and to perform normal hygiene procedures without changing the dressing.
Therapeutic proceedings (including the selection of a dressing) and the cost depends on the type of wound and the stage of healing . Some wounds are treated for many months, sometimes over a year. There are often problems in the healing process, and the most dangerous of them cause infections. An unsecured wound may be infected with bacteria, viruses or fungi. They proliferate spontaneously and poison tissues with their secretions. The wound infection can spread quickly up to the form of sepsis, which threatens the patient’s life. The cost of treating infected chronic wounds significantly increases mainly due to the need to use more specialist dressings and the use of expensive antibiotics.
As a national consultant I observe with great concern that the number of people who suffer from pressure ulcers and other chronic wounds is not decreasing despite years of educational campaigns. The responsibility for this situation falls not only on the nurses but also on those responsible for creating the conditions for the care of sick and dependent people, and the National Health Fund as a payer financing the costs of treatment. It is difficult to understand the fact that the National Health Fund does not require health care centres to report on patients with bedsores and the course of treatment. Isolating procedures concerning the treatment of bedsores, and leaving the treatment costs within the institution in which they occur, would highly affect and activate the creation of suitable conditions for the prevention of pressure ulcers. It should of course take into account the fact that some chronic wounds are not the result of negligence but result from the patient’s physical condition; most often it relates to end-phase of long-term biologically devastating neoplastic disease.
As part of my own professional practice I was able to watch quite remarkable effectiveness of modern specialised dressings in the treating of pressure ulcers. Of course, the nurses should be aware of all the known methods of chronic wounds treatment, not only of pressure ulcers but also ulcers, malignant ulcers, diabetic foot ulcers and burns. The bottom line is to be aware that it is unacceptable not to obey the basic prevention principles and to expose the patient to the formation of pressure ulcers or other chronic wounds. Both health and financial consequences of economising on absorbent products and protective dressings are very serious, not only for the patient but also for the nurses and the unit they work for.
Elżbieta Szwałkiewicz
National Consultant in Nursing Chronically Ill and Disabled People
Even the most modern, well-matched to the wound type dressing will not facilitate the wound healing process if additional conditions conductive to further body regeneration will not be met.

These are:
- proper body hygiene,
- skin protect against irritating effects of urine,
- suitable bed, mattress, bed linen and underwear,
- elimination of pressure on the part of the body affected by a bedsore,
- safe movement and positioning of the body,
- adequate nutrition and hydration.
Modern technical solutions and technologies allow for the safe performance of hygienic activities, even in those patients with very sensitive skin and completely immobilised, without the risk and effort associated with their movement. On the market there is a wide range of skin care, hygiene facilitating devices available. When dealing with dry skin (frequently washed with soap), weakened, macerated, constantly subjected to the action of irritants, it is necessary to check the condition of the skin daily looking for signs of an allergic reaction. Appropriate preparations for cleansing and skin care of the sick are the ones that can be applied to sensitive and irritated skin, and have moisturising, greasing and elasticising properties. They should alleviate symptoms of inflammation, grease and protect the skin against irritants such as urine. For irritated and itchy skin soap should not be used only mild cleaning agents (lotions, foams). It is advisable to use cosmetics with as little allergic reactions as possible. The used cleaning and care products should be manufactured in sets by the same company as this will prevent the use of products of different chemical components coming into harmful interactions for the organism. Just wash the wound area, and always check the condition of the wound dressing and protection of the wound against pollution and getting wet during hygiene procedures.
Unpleasant for the patient and his/her environment urine odour can be eliminated by proper selection of absorbent materials and their appropriately frequent change – about four times a day. While changing be sure to cleanse the abdomen, genitalia, groin and buttocks.
A patient who cannot change the position from lying to sitting can be washed traditionally in bed, but can be also bathed in a special movable bathtub. The bathtub is taken into the patient’s room, one side wall is removed and is set along the bed. Then, using a cloth or a special sliding mat to move the patient (previously undressed and covered) into the tub. If the patient is on a drip, monitor, respirator, etc., the bath is carried out in the room next to the bed. This is possible when to the sink tap (located in the room) a shower hose of suitable length with a shower head is attached. Similarly, the drain hose must be of appropriate length to reach to a special outlet installed under the sink. If the patient is able to leave the room, he/she is taken on the bathtub to the bathroom with a shower post. The drain hose is introduced into the floor drain. Bathing in the supine position can also be done in a bathtub with an adjustable height. A person who cannot move, is moved (undressed and covered) by sliding onto a special man lift – a kind of trolley-stretcher. Following the transfer of the patient to the bathroom, the lift is placed on the bath, which rises (electric mechanism operated by means of a remote control) to the height appropriate for the carer, so that he/she does not to have to bend down. Then, the lift with the patient is lowered to the bottom of the tub. Most of the mentioned bathtubs has also an incorporated hydro massage device. The lift has the ability to raise the head rest so that the patient can be washed in a sitting or reclining position. In a set with the bathtub there are also available chair lifts that help people with paraplegia or the disabled to get to the bathtub and leave it. These people can also wash themselves in the shower using the lift or a sanitary chair. All institutions where there are patients with locomotor disabilities should have integrated systems for personal hygiene i.e. movable equipment integrated with cleaning equipment.
People unable to walk e.g. with paraplegia can use the toilet alone but there must be conditions created enabling the move from the wheelchair onto the toilet. The height of the toilet and the wheelchair should be similar. The side walls of the chair and security handles at the toilet should be tippable. Within easy reach of a person using the toilet there should be a shower head to wash and toilet paper to dry the skin. The ability to wash oneself with running water is highly important, because it is very difficult to clean the genital and anal area with toilet paper. In elderly people the skin is wrinkled and therefore its thorough cleaning off stool remnants is not possible by means of dry toilet paper, and repeatedly rubbing the sensitive and dry skin often leads to its damage. In the toilet there should be enough space for a disabled person to drive a wheelchair, park along the toilet, and after picking up the side part of the chair and the toilet handle, move onto the toilet. All people, regardless of their health and fitness, should be able to use the toilet. It should be kept in mind that when lifting and moving the patient strong point pressure on the body ought to be avoided and the sliding method to rotate the body ought to be applied. The need to clean and protect the skin is particularly important for people with disabilities who face the problem of urinary incontinence.

Please note that urine in contact with the skin is an external irritant, causing inflammation. The inflamed skin is red, irritated and painful. There appears also often swelling, itching and flaking of the skin. Patients trying to reduce the annoying itch scratch themselves, and ultimately break the continuity of the skin, leading to the formation of wounds. These scratches are the site of bacterial infection and the development of complex infected bedsores.
The desired effect can be achieved using hygienic disposable absorbent materials, sets for urine collection, specialist personal hygiene and cosmetic and protective preparations. Their offers is very rich in the market.
Diapers, anatomically shaped diapers or urine pads should be chosen according to their absorbent ability, the content of a urine binder, the type of protection against the leakage from the diaper, the ability to reduce unpleasant odours and the possibility to closely adjust to the body. It is also important that the absorbent body is covered with special nonwoven, which also separates the urine absorbed from the skin.
Urinary incontinence leads to constant moisture and maceration of the skin, which promotes its inflammation, damaging, resulting in the formation of bedsores. Therefore, it is necessary to systematically check the condition of the skin in areas exposed to moisture and the state of dressings, and maximally shorten the time of skin contact with urine.
Therefore, the selection of an absorbent product should be determined by the degree of urinary incontinence, the patient’s level of consciousness, time of the day and level of activity. People with pressure ulcers or very sensitive dry skin prone to irritation, should use the so-called breathable diapers. They differ from other diapers for instead of the protective film they have to a special air-permeable laminate.
While nurturing a bedridden person with urinary incontinence (UI) it necessary to use hygienic underpads to maintain the cleanliness of linen or to secure the chair. Do not use rubber underpads but pads made of cellulose with one side coated with special film protecting the chair or the bed against wetness. Here also breathable absorbent products should be applied. People with bedsores should avoid overheating in warm clothes and airless or overly heated rooms, and above all, they should avoid long-term pressure on the damaged skin and skin friction over the ground. This effect can be achieved by using a special sliding and equipment for sliding repositioning, pressure relief mattresses and pillows, frequent change of body position, the application of proper rules for lifting and moving the patient.
Significant reduction or elimination of pressure on the skin can be achieved by equipping the bed with an anti-bedsore mattress:
- alternating pressure (so-called dynamic) anti-bedsore mattress where a motor pumps air into individual chambers of the mattress, filling them only some of them which allows to temporarily relieve another part of the body. Using the mattress does not cancel the obligation to adequately frequent change body position.
- constant pressure anti-bedsore mattress, pumped using a hand pump, enabling to achieve appropriate pressure and reduce the pressure on the body surface. It is also important that it is made of a material with a unique antibacterial formula inhibiting the growth of bacteria and odour inhibitor. Using this mattress has a preventive effect and accelerates healing of existing wounds. This mattress is particularly useful in patients who dislike the sound of the pump motor in the dynamic mattress.
The time of healing a bedsore or any other chronic wound depends on the general state of health and on good nutrition with adequate supply of protein, calories and fluids.
Causes
The diabetic foot syndrome deals with changes appearing on the lower extremities in patients with diabetes.
The cause of the diabetic foot syndrome are changes in the blood vessels (ischemia), and damage to the nerves (neuropathy). Deterioration of vascularisation and innervation in diabetic patients usually progress simultaneously, but only one of these changes is dominant. The dominant factor determines the type of the diabetic foot syndrome, and so can be distinguished: ischemic diabetic foot syndrome or neuropathic diabetic foot syndrome.
Figure: diabetic foot syndrome – classification as for the dominant factor
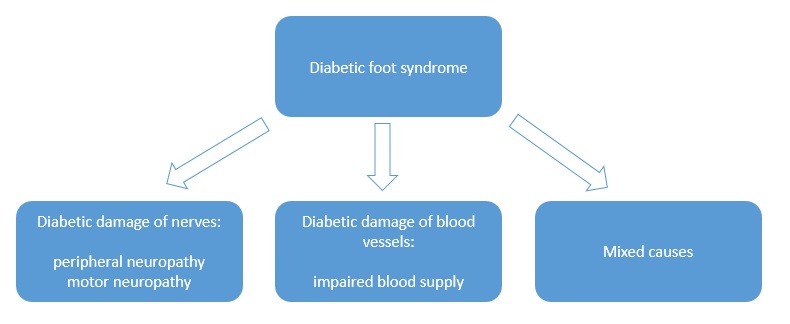
Peripheral neuropathy i.e. peripheral neuritis – is one of the complications of prolonged hyperglycemia and affects both somatic and autonomic nerve cell projections in both legs. The patient has reduced sensation of pain, temperature and touch in the affected leg, and since feels no pain after an injury or compression, the skin is often damaged and ulcers are formed, which are often not noticed early enough and thus start to be treated too late. Late detection of the ulcers may be then too advanced to be successfully treated.
Motor neuropathy causes loss of muscle and foot tendons and, consequently, destruction of the joints. This in turn leads to the concentration of workload on a few small areas of the plantar surface, and further to the formation of callus. The final step of these changes is foot deformation.
Angiopathy i.e. damage to blood vessels – blood supply disorders are characterised by abnormal blood flow in the legs especially tibial and fibular artery. Uncontrolled diabetes favours the development of arterial diseases. The control of blood glucose content is one of the prevention ways, it is also a precondition for starting the process of wound healing.
Therefore, we can distinguish:
- neuropathic foot ulcers, which constitute two thirds of all diabetic foot ulcers
- angiopathic foot ulcers (~ 10%)
- mixed foot ulcers (~ 25%)
Risk groups
- People with diabetes mellitus.
- People with undiagnosed diabetes!
This disease affects mostly people with type II diabetes i.e. the one not requiring insulin injections.
The complication in for of diabetic foot is present in approximately 20% of hospitalised patients because of diabetes, and is the cause of 50% of all limb amputations performed in surgical wards.
Symptoms
Neuropathic diabetic foot
The predominant symptoms:
- loss of sensation to touch, pain and temperature
The patient does not feel the presence of a malicious stimulus such as a cut, burn, hurting by wearing tight shoes, the presence of a foreign body in the shoe. Insensitivity to pain is the basic element causing the formation of ulcers on the foot sole. The neuropathic diabetic foot is warm, with preserved flow in the arteries, but the foot joints and bones are deformed.
In some patients the changes appear in the joints and are formed by gradual destruction of small joints of the foot which results in considerable distortion of the feet. It is necessary then to wear special shoes made upon an individual order. Wearing normal ill-fitting shoes very often leads to the formation of ulcers.
Ischemic diabetic foot syndrome – angiopathic
The predominant symptoms:
- increased sensitivity to pain
The main symptoms are: pain intensifying usually at night, often accompanying painful muscle cramps, tingling or numbness in the leg.
Depending on the level of stenosis and occlusion of arteries in the lower limb, necrosis appears on different areas of the foot.
The most severe form of the disease is the closure of large arteries in the lower limb above the knee. This results in tissue necrosis in the foot, and sometimes also in the lower leg. Necrosis affects mostly toes. Ischemic diabetic foot is characterised by preserved innervation while simultaneous impaired blood supply in the limb.
An untreated diabetic foot syndrome leads to the amputation of the limb.
Location
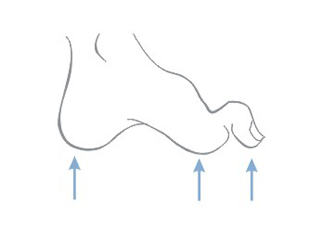
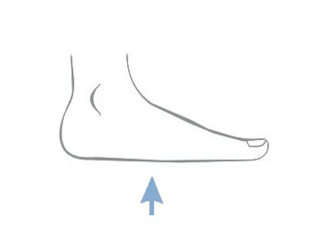
In patients with diabetic neuropathy ulcers are located primarily in areas of repeated injuries and affect usually the plantar surface of the foot around the metatarsal bone, heel and toes. Usually the neuropathic ulcers are painless.

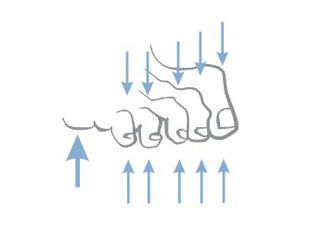
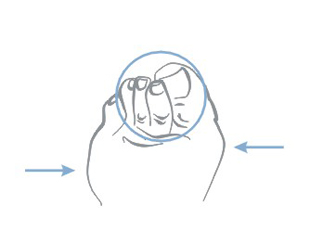
In addition, as a result of neuroarthropathic disturbances, the foot is distorted in a characteristic way – grooved feet, mallet toes, changed way of walking, and in over-loaded points in the calluses (corns) are formed that can later cause non-healing wounds and ulcers.
In the case of ischemic diabetic foot chronic hypoxia causes that the foot begins to die – it swells, ulcers, necrosis and cracks appear, nails get deformed and soft tissues disappear and the whole foot becomes blue.
Treatment
A specialist in the field of diabetes, surgery (including vascular surgery) and orthopaedics is the competent person for ordering treatment. Nurses also actively participate in the therapy. The most important thing is to keep sugar level in blood in optimal physiological limits.
The treatment is both causal and local.
Wounds are surgically debrided, narrowed blood vessels are unblocked, various vascular grafts are used to allow bypass clogged arteries which improves blood flow in the foot. Along with the surgery blood sugar in the body is controlled and medicaments facilitating the treatment are dosed. In addition to insulin and antibiotics the patient receives medicines that improve blood circulation in the limbs, reduce blood viscosity, enabling to reach the ischemic structures, improve wound healing and scarring. Also appropriate diet is recommended.
Prevention
It most essential in the prevention of diabetic foot development is the proper treatment of diabetes, the control and maintenance of a normal blood sugar level.
After diagnosing diabetes the patient should:
- quit smoking
- gently and carefully take care of the feet
- systematically control the circulation and innervation of the feet
If there are foot lesions, early physician intervention often prevents the need of amputation of the lower limb.
Everyday foot care in people with diabetes should consist of:
- everyday observation – controlling blood flow and sensation, washing in warm (not hot) water, gentle and careful drying – especially the space between toes
- care for nails – regular trimming (but not too short)
- careful selection of shoes – should be sufficiently wide, the right size (patients with neuropathy, due to the worsening of sensation tend to buy too small shoes, smaller than the ones worn so far), the heel should be low and wide, shoes with laces are recommended
- before putting on shoes the patient should check whether inside there are no sharp objects, outstanding seams or rolled inserts
- wear non-binding and non-elasticated socks made of natural fibres (too tight socks can impede blood circulation)
- protect the foot against excessive: soaking , exercises or heating (for example by means of an electric blanket or other energy sources)
- do not use ointments on foot corns – unless your doctor tells otherwise
Any observed changes in the foot, such as swelling, colour change, loss of sensation should be consulted as soon as possible with a doctor.
Even minor cuts, skin cracks and wounds cannot be ignored and always need to be secured with sterile dressings and shown to the doctor during control visits. If there is no progress in the healing it is recommended to urgently consult the doctor.
>
Causes
The causes of leg ulcers are diverse, internally complex and almost exclusively of endogenous-internal origin.
Without a doubt, however, the most common cause of leg ulcers is venous hypertension and arterial insufficiency.
Other possible causes of leg ulcers:
- hypertension: necrotising vascular dermatitis – necrotic angiodermatitis (Martorell syndrome)
- infections: osteomyelitis, tuberculosis, pyoderma gangrenosum, leprosy, insect bites
- vasculitis: polyarteritis nodosa, rheumatoid arthritis
- haematological disorders: haemolytic anemia, fibrinolytic disorders
- neurological disorders: poliomyelitis, peripheral neuropathy (diabetes)
- cancer: mixed basisquamous carcinoma (Marjolin’s ulcer), melanoma, Kaposi’s sarcoma, lymphoma
Ooccurrence
- 75% of all vascular ulcers are the result of venous hypertension – venous ulcers
- 15% is generated as a result of atherosclerosis – mixed ulcers
- 10% is arterial ulcers
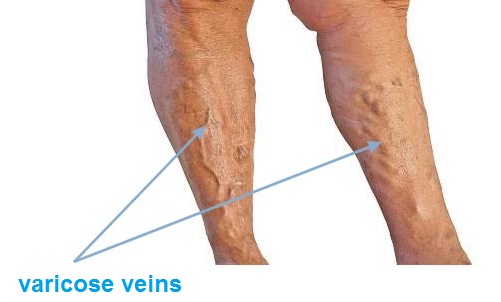
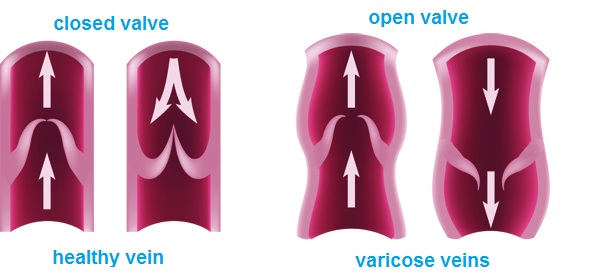
Venous ulcers are caused by severely impaired activity of leg veins. In advanced venous insufficiency of the lower limbs, venous circulation in the lower limbs is disturbed and venous valves are damaged – which results in congestion and increased pressure in the veins. Valves control the blood flow so that it flows only in the direction towards the heart, not to move back. In case of damage or malfunction of valves blood flows back to the lower limb. Blood pressure in the venous system increases, which, if untreated, causes further damage to the valves and superficial veins. Walls of veins lose their flexibility and elasticity, get thicker. For the purpose of treatment and prevention of recurrence of ulcers, it is very important to identify the locations of venous insufficiency.
Risk group
- obesity
- work in a seated or standing position, leading to the stagnation of blood in leg
- hereditary factors – presence of varicose veins in parents
- age, mostly at risk are people over 60 years of age
- sex, statistically varicose veins are more common in women than in men
- number of pregnancies (the more births the greater the risk of varicose veins)
- constipation
- flat feet
- oral contraception
- tallness
Symptoms
The initial phase of venous insufficiency: feeling of heavy legs, especially in the evening, the emergence of the so-called spider veins and reticular veins. The next stage in the development of the disease are: emerging swelling around the ankles, then also swelling of the entire lower leg. Initially the swelling disappears after a night rest, and then becomes constant. After some times varicose veins may occur i.e. permanent extension of superficial veins.
In advanced venous insufficiency of the lower limbs trophic skin changes appear as well as discoloration, spots and hardening. Then itching appears, bumps, cracks, skin covering varicose veins is damaged, which inevitably leads to the formation of difficult to heal wounds known as leg ulcers.
Location
- Typical venous ulcers are located above the medial malleolus leg.
- Ischemic ulcers (arterial) are often found on the back of the toes, on the heel, or on the front surface of the shin.
- Rheumatic ulcers usually involve the side and back surface of the rest of the lower leg and the ankle area.
Where to seek help and advice
Of course, in the first instance go to your GP who should refer you to a specialist surgeon. Currently, the best method of diagnosing venous insufficiency is to perform an Colour Doppler ultrasound test.
Treatment
In case of ulcers resulting from advanced chronic venous insufficiency, leg swelling, not treated varicose veins, it is a standard to conduct a multidirectional model of treatment comprising of:
- local treatment of the wound – treatment by means of dressings,
- compression therapy – treatment with special bandages or stockings,
- drug therapy – treatment with pharmaceuticals – medicines,
- and ultimately the elimination of venous reflux – surgical treatment.
The local treatment is to accelerate the cleansing of the ulcer from necrotic tissue and stimulation of the healing process. The purpose of the conservative treatment is to reverse the effects of venous hypertension, improving venous return, and thus – reducing the swelling. The basis of the conservative treatment is the compression therapy. It increases local hydrostatic pressure and reduces pressure in superficial veins, reducing the transudation of fluid from the blood. Gradual compression accelerates blood flow in the veins of the deep system. An extremely important element of the conservative treatment is the pharmacotherapy.
The treatment of leg ulcers is tough and long-lasting, so to make it the least expensive and effective it must be based on genuine and systematic cooperation with a healthcare professional.
Prevention
Factors which a person can control are WEIGHT and LIFESTYLE.
WEIGHT:
- losing excess weight
LIFESTYLE:
- increasing physical activity especially walking, cycling, swimming. This activities the so-called “calf pump”. Muscle contractions stimulate the venous circulation, pushing blood to the heart – blood does not stop in the veins.
- taking care of yourself in the workplace, especially when staying seated – footrests, avoid staying long in one position without moving or standing. Involving exercises allowing the calf muscles to work – for example, march in place in an upright position, bending towards the foot being in a sitting position.
Once microcirculatory disturbances occur, they can be corrected through the use of compression products:
- knee-socks
- stockings
- anti-varicose tights
and involve medical treatment – always preceded by consultation with your doctor or a pharmacist.
Maria T. Szewczyk, Ph. D.
Department of Surgical Nursing, Ludwik Rydygier Collegium Medicum in Bydgoszcz, Nicolaus Copernicus University in Toruń
In the treatment of ulcers, especially of their advanced form, omnidirectional and interdisciplinary care of the patient is required. Venous ulcers are chronic wounds, where the healing process is difficult and lengthy, and requires the effort of many measures. (…)
Chronic venous insufficiency and venous ulcers
In about 80% of cases the cause of leg ulcers is chronic venous insufficiency. Venous ulcers are the final and most serious complication. In the treatment of ulcers, especially of their advanced form, omnidirectional and interdisciplinary care of the patient is required. Venous ulcers are chronic wounds, where the healing process is difficult and lengthy, and requires the effort of many measures. Extensive and ongoing for years wounds often lead to movement limitation in the ankle joint, foot deformation and permanent disability (Photo 1, 2, 3, 4).

(archive of the author)

(archive of the author)

(archive of the author)

(archive of the author)
The first step is the diagnostic and ultrasound examination of venous vessels, and then topical and causal treatment. Etiopathogenesis, in which the main role plays venous hypertension, requires at first elimination or reduction of causative factors. The cause of ulcers are in fact circulatory disorder leading to the venous hypertension in the lower limbs. These relate to pathological anatomical and physiological changes occurring in several successive stages. It begins with overload and baggy or fusiform enlargement of the vascular system in the form of varicose veins. Accompanying changes include: a decrease of flexibility and patency of blood vessel walls, and valvular regurgitation, venous blood reflex and (or) occlusion of the deep venous system (by e.g. deep vein thrombosis). Long-lasting high hydrostatic pressure eventually leads to an increase in vascular patency and transition – first of exudate and also of cellular components. In the so-called gaiter area of the leg (the lower half of the leg above the ankle and around the ankle) trophic changes occur, initially only in the form of over-pigmentation and discolouration, and later also in the form of inflammation, fibrosis and thinning of the skin tissue. On the surface of these changes ulceration can be developed. The immediate cause of the injury can be not only the changes in the skin nutrition, but also spontaneous rupture of varicose veins, or even a slight mechanical shock.
The gold standard of conservative treatment of venous ulcers is compression therapy followed by wound cleansing and active moist or biological dressings.
Compression therapy
In the conservative treatment a vital role plays compression therapy, which deals with individually chosen compression dressings. It can be bandages (band) with compatible compression degree as well as ready products in the form of knee-length, short and long stockings and tights. The compression therapy using the bandages depends inter alia on the material from which they are made and the method of bandaging the limb. The use of the compression greatly reduces venous hypertension in the superficial system, improves the efficiency of the muscle pump, reduces venous stasis and restores proper hydrostatic conditions for the outflow of blood from the vessels. The compression will be effective if the degree of compression will be applied depending on the severity of chronic venous insufficiency i.e. it will depend on the superficial, perforator and deep vein system. To measure the interfacial pressure of the compression a Kikuhime device is used. With the help of this apparatus we can provide the required pressure. (Photo 5)

(archive of the author)
Similar effects can be brought by a massage – both sequential pneumatic massage (Photo 6) and manual massage reducing the oedema and improving the return of venous blood towards the heart.

(archive of the author)
Before the use of compression the state of the peripheral circulation must be checked. The use of compression therapy in a patient with impaired blood flow can result in severity of ischemia, skin necrosis, and even limb amputation. Therefore, before applying the compression therapy is necessary to perform Doppler imaging and marking the Ankle Brachial Index (Photo 7).

(archive of the author)
Topical proceedings
The topical proceedings parallel with the compression therapy includes: necrosis removal, wound debridement, moist wound healing, care of the skin around the wound.
Contaminations, superficial necrosis reaching the dermis can be removed in a conservative way, e.g. mechanical, enzymatic, autolytic, and in a surgical way. However, necrotic tissues, including subcutaneous layers require a surgical intervention by removal of the changed tissues with a scalpel and scissors. You can also include the VAC system (vacuum-assisted wound closure) as a non-invasive active therapy to promote healing in difficult wounds that fail to respond to established treatment modalities. The method of necrosis removal is determined by the location and depth of the ulcer, the exudate amount in the wound and the patient’s general condition. Of great importance in the selection of the treatment method is the nature and extent of necrosis structures. The mechanical wound debridement, as well as the surgical debridement of wound edges give immediate effect to remove necrotic elements. The autolytic debridement is a natural process that occurs spontaneously in a properly healing wound. It is the effect of proteolytic enzyme and phagocyte activity , which can be both initiated and supported by the maintenance of moist environment at the bottom of the wound. Low severity of these processes in the debridement phase might require to use ready proteolytic enzymes and to introduce enzymatic debridement. Wound cleaning and removal of the necrosis reduces the risk of infection and the development of a local infection. The purpose of this treatment is to prepare the wound to further proliferative processes and stimulation of these processes to maintain optimal healing conditions. Please note that venous ulcers are heavily exposed to the risk of infection. It can be caused by different types of microorganisms (viruses, bacteria and fungi), but the most common etiological agent are bacteria, including staphylococci, streptococci, Escherichia coli and Pseudomonas. Proliferating in the wound, the bacteria secrete its own metabolites and toxins, destroying migrating fibroblasts and budding vessels, and limiting the healing progress. An uncontrolled infection can spread deep inside the wound, infiltrate adjacent tissues, and even lead to the development of sepsis.
The risk of infection and the development of infection can be additionally reduced by flushing the wound bed with antiseptic solution. Its concentration should not only have a bactericidal or bacteriostatic effect, but also should be safe for healthy tissue and does not cause cytotoxic effects or inhibit the healing. Only the preparation meeting the above criteria can be safely applied directly on the wound surface (e.g. Octenisept containing a mixture of octenidyne dihydrochloride and phenoxyethanol safe for skin and mucous membranes). In justified cases general antibiotics are used, which should not be used topically. To support the natural debridement and recovery processes, on a clean wound a special active dressing maintaining moist wound healing environment should be applied.
Moist wound healing
Features of the “ideal” dressing, developed on the basis of Winter analysis (1962) and his successors are satisfied by so-called new generation dressing. They maintain adequate moisture wound environment, which prevents the scab formation and drying out of the ulcer surface. A moist wound heals twice as fast and in a more structured way, because the moist environment stimulates both cell proliferation and the migration of new cells, ensuring their optimal differentiation and neovascularisation.
Features of a dressing supporting the natural healing processes were defined in 1991 by Turner et al:
- maintains a moist environment in the wound bed,
- has high absorption capacity, regulates the excess of exudate,
- does not adhere to the wound surface, enables painless and atraumatic change,
- protects the wound against bacteria and contamination,
- is non-toxic and non-allergenic,
- maintains the correct wound temperature similar to the body temperature,
- facilitates the healing process at all wound healing stages.
The new generation dressings fulfilling the listed criteria are produced in several groups, differing in the design and application. They are designed for different types of wounds, depending on their etiology, the healing phase, the depth of tissue damage, the nature of the exudate and the presence of an infection.
The dressings have different properties to keep the exudate, whose secretion varies during the particular wound healing phases. Apart from the outer protection and moisture content control the dressing has to fulfil other important task at every stage of venous ulcers healing.
Skin care
The management of chronic venous insufficiency in states with weak skin barrier function requires particularly attentive care and concentration of efforts aimed at conditioning and regeneration of the natural protective barrier of the epidermis. One of the major care actions taken in concern of the integrity of the skin is to maintain the cleanliness of the body, including the limbs. Cleaning agents used for personal hygiene should be properly chosen and correctly applied, especially when it comes to this group of patients. Detergents are designed to remove and reduce the number of contaminations and microorganisms residing on the surface of the body, if possible without damaging the skin protective barrier. Since the lipid coat has the properties of “binding” impurities, and water alone is not able to overcome them, the washing agent needs to contain surfactants. It is recommended to use agents that are delicate, have a pH of 5.5 or liquid agents containing a substance modifying the acidity of the product (for example: phosphoric acid, citric acid, sodium hydroxide, triethanolamine), and enriched with physiological lipids, ceramides, and moisturising agents, which at least partially allow to compensate for the lipid loss caused by the action of the detergent.

(archive of the author)
After thorough cleaning of the skin it is advised to apply agents supporting the regeneration and increasing the moisture level of the skin. This can be obtained thanks to biologically inert substances supporting the treatment and skin care of the, so-called emollients. Due to moisturising properties, they increase the water content of the stratum corneum and improve the biophysical properties of the epidermis (Photo 8). The emollients are available in form of creams, lotions, ointments and emulsions of different consistency, serving the same purpose – moisturising and / or oiling the dry skin. Creams and ointments usually need to be applied thicker. Agents of lighter consistency, such as lotions, make it possible apply thin film. Agents applied on sensitive skin should not contain alcohol, metals, fragrances, or talc. In specific situations they should contain only water-based hydrophilic ingredients. Distributed on the skin they are easily absorbed, and after washing do not leave unwanted residues.
Literature:
- Benbow M, Burg G, Comacho Martinez F, et al. Guidelines for the outpatient treatment of chronic wound and burn. Blackwell Science, Berlin-Vienna 1999, 12-21.
- Szewczyk MT, Jawień A.: Chosen aspects of conservative treatment of venous ulcers. Part I: Compression therapy. Progress Dermatol. Alergol. 2005, XXII, 3: 133-140.
- Blair S, Wright D, Blachkouse C, et al. Sustained compression and healing of chronic venous Ulcers. Br Med J 1998, 298: 1159-1161.
- Ciecierski M, Jawień A. Clinical picture of chronic venous insufficiency. Medical guide 2004, 8 (68): 36-48.
- Hess CT. When to use hydrocolloid dressing. Nursing 1999; 29.11: 20-23.
- Szewczyk MT, Jawień A, Piotrowicz R. Treatment of venous ulcers. Medical guide 2004, 8 (68): 66-71.
- Szewczyk MT, Jawień A, Piotrowicz R. The use of compression therapy in venous diseases. Medical guide 2004, 8 (68): 58-64.
- Jawień A. Szewczyk MT. (red) Venous leg ulcers. Ed. Your Health. 2005.
- Jawień A. Szewczyk MT. (red) Clinical and nursing aspects of care for patients with venous ulcers. Termedia 2008.
- Szewczyk MT., Mościcka P., Cwajda J. et al Evaluation of the effectiveness of new polyurethane foam dressing in the treatment of heavily exudative venous Ulcers. Acta Angiol. 2007 T.13, 2: 85-93.
- Placek W. Role of substrates and emollients in the prevention and restoration of the epidermal barrier. Aesthetic Dermatology 1999, 4: 174-178.
- Korinko A. Yurick A. Maintaining skin integrity Am J Nurs 1997 (2): 40-44.
- Wojnowska D., Chodorowska G., Juszkiewicz-Borowiec M. Dry skin – pathogenesis, clinic and treatment. Advances in Dermatology and Allergology, 2003, XX, 2: 98-105.
- Szewczyk MT, Jawień A. Recommendations of specialised nursing care of patients with venous leg ulcers. Surgical and Vascular Nursing 2007, 3 (1): 95-129.
Causes
The cause of pressure ulcers (also called bedsores, decubitus ulcers or pressure sores) is tissue ischemia due to the prolonged pressure evoked on veins and arteries.
The risk of pressure ulcers depends on the duration of the pressure – the longer the pressure is present or the greater the force, the greater the possibility of developing bedsores.
In healthy people prolonged pressure causes pain forced to change position.
Unconscious and immobile people are not able to relieve the pressure automatically and to improve the blood circulation, thus they belong to the group of people at increased risk of pressure ulcer development.
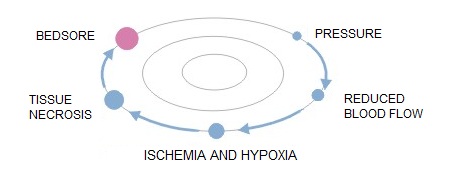
Pathomechanism of developing bedsores:
- simple pressure i.e. the pressure exerted on the soft tissue on one side by the bone, and on the other by a hard surface
- rubbing the patient’s body surface over bed linen e.g. when using improper technique for changing positions
- lateral tensile forces, which act directly on the patient’s body
Risk group
The risk of developing pressure ulcers should be considered in all patients with long-term reduction of capacity for self-movement, which spend most of their time in bed or in a wheelchair.
Factors that increase the risk of pressure ulcer development are:
- age
- weight
- nutritional status
- sphincter function of the urethra and the anus
- state of consciousness
- diabetes, atherosclerosis
- steroid therapy
Symptoms
Pressure ulcers are classified according to the severity of the symptoms into 4 or 5 degrees. And hence:
- Stage I: intact skin with non-blanchable redness of a localised area usually over a bony prominence. The area may be painful, firm, soft, warmer or cooler as compared to adjacent tissue. Microcirculation is not damaged yet.
- Stage II: partial thickness loss of dermis presenting as a shallow open ulcer with a red pink wound bed, without slough. Presents as a shiny or dry shallow ulcer without slough or bruising.

- Stage III: abrasions, cracking skin and full-thickness skin damage to the border of the subcutaneous tissue, blisters, the wound edges are well marked out, surrounded by edema and erythema

- Stage IV: the damage extends towards the subcutaneous fatty tissue; the ulceration can be free from infection and necrosis and covered with clear granulation tissue, but the necrosis may also affect the fatty tissue and the surrounding skin layers. The bottom may be covered with black necrosis.
- Stage V: the presence of advanced necrosis, which extends towards the fascia and muscles; the damage can also affect joints and bones – unpleasant odour and profuse pus-necrotic discharge; in the wound there are pieces black dead tissue and black necrosis

Location
Bedsores occur in places where the distance between bone prominence and the skin surface is the smallest i.e. in contact point of the skin and the ground, where the pressure is the highest. Most pressure ulcers are formed around the aitchbone, coccyx, buttocks, on the heels or the hips.
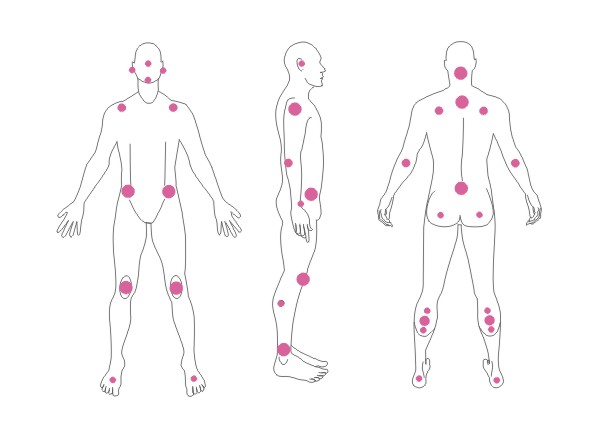
The above figures present the point of contact of the skin with the surface at various positions of the patient laying on the bed.
Where to seek help and advice
Of course, in the first place consult the general practitioner.
The treatment of pressure ulcers is the responsibility of a doctor and a nurse who has completed a specialist course in the treatment of chronic wounds. The competences of nurses are limited to the treatment of pressure 1 to 3 degree sores.
Sometimes the condition of the wound requires surgical debridement and then the GP directs us to a specialist surgeon.
The treatment of pressure ulcers is tough and long-lasting so to make it the least expensive and effective it must be based on genuine and systematic cooperation of the doctor and the patient, and must be combined with an intensive, professional care.
Treatment
First of all the treatment should be conducted under the supervision of a doctor or a nurse.
Bedsores are treated locally i.e. the wound is to be secured with dressings appropriate.
A very important part of treatment is also appropriate patient care, which include:
- position changing – the patient should not lie on the bedsore
- placing patient on a pressure relief mattress
- protecting sore places with special anti-bedsore discs and stands
- adequate nutrition and hydration of the patient
- controlling comorbidities
The most effective form of treatment is the use of specially designed wound dressings for this purpose, the so-called specialised or advanced dressings that create a moist wound healing environment.
Choosing the right, effective dressing it must be based on a correct diagnosis of the processes occurring in the wound. To make it easier, you can use the wound colour classification matrix, which is based on the observation of the phenomena that take place in different phases of healing.
Wound colour classification matrix:

Black wounds

Wounds with black necrosis require:
- maintaining a moist environment
- removal of necrotic tissue in order to initiate the healing process
The healing process will not occur under thick layers of necrotic tissue; to begin it first the necrosis needs to be removed. We have a choice of two basic ways to get rid of the necrosis from the wound bed:
- surgical debridement – the mechanical removal of necrotic tissue to expose healthy skin structures for initiating the process of wound healing
- application of interactive dressings – involves the application of dressing on a wound, which stimulates the autolysis process i.e. the natural wound cleansing by the body. In this case the necrosis decomposition is made by enzymes produced by the damaged wound cells.
Recommended dressings for black wounds:
- Medisorb G – hydrogel dressing
Yellow wounds

Wounds with yellow, colliquative necrotic tissue require:
- maintaining a moist environment
- absorbing excess exudate, along with the remnants of necrotic material
Wounds with colliquative necrosis are characterised by an increased exuding level. The necrosis on the bottom of the wound is liquid. Such wounds provide an ideal environment for the growth of microorganisms, and therefore they are often infected. The tasks for the dressing in this case is the absorption of exudate and necrotic material, liquefaction of too dry and too dense necrosis, protection against drying out and against secondary injuries.
Recommended dressings for yellow wounds (depending on the exudate level and the depth of the wound):
Medisorb A – alginate dressing – heavy or moderate exuding wounds; superficial and deep wounds
Medisorb P – absorbent dressing – heavy or moderate exuding wounds; superficial wounds
Medisorb H – hydrocolloid dressing – moderate and low exuding wounds; superficial wounds
Red wounds

Red wounds with visible granulation tissue required:
- maintaining a moist environment
- protecting against secondary infections
- controlling the exudate level
Apart from maintaining a moist environment, these wounds also require protection against possible mechanical injuries. This is particularly important since a well-vascularised granulation tissue is susceptible to injuries which delay the healing process and can be the source of infection. Another important factor is to maintain the proper temperature (close to body temperature), so that new cells can grow at optimum speed.
Recommended dressings for red wounds (depending on the exudate level and the depth of the wound):
- Medisorb A – alginate dressing – heavy or moderate exuding wounds; superficial and deep wounds
- Medisorb P – absorbent dressing – heavy or moderate exuding wounds; superficial wounds
- Medisorb H – hydrocolloid dressing – moderate and low exuding wounds; superficial wounds
Pink wounds

Pink epithelising wounds require:
- maintaining a moist environment
- protecting sensitive tissues
When the wound begins to cover with epidermis it needs to be protected against drying out, friction and other factors that could damage the newly formed tissue.
Recommended dressings for pink wounds (depending on the exudate level and the depth of the wound):
- Medisorb H – hydrocolloid dressing – moderate and low exuding wounds; superficial wounds
- Medisorb F – film dressing – low exuding wounds
The analysis of wound healing phases shows that wounds being at various stages of healing, require some other conditions for the process to run smoothly. It is important to remember that in addition to various healing stages, the wounds are also varied because of the size, depth, presence of necrotic tissue and exudate level. All these features result in the fact that each wound requires the selection of the right kind of dressing, sometimes even a few dressings that will change during the healing process.
The following table presents factors that may slow down the healing process.
Table: Factors slowing down the wound healing process
| slowing down factor | why | optimum conditions | how does it work in optimum conditions |
| dry environment | moist environment | appropriate level of wound exudate: allows activation of natural wound debridement; accelerates granulation; provides quick and correct course of epithelisation | |
| necrotic tissues | wound healing is possible only after the removal of dead tissues; the necrosis may be a substrate for the development of infection | curgical / autolytic wound cleansing | cleansed the wound enable the begin of the granulation phase |
| infection | all mechanisms in the wound tend to fight the intruder; the healing process is hampered | fight infection | cleansed the wound enable the begin of the wound healing process |
Prevention
Basic rules:
- systematic change of body position every two hours and reduce pressure in places at risk, through the use of special pressure relief mattresses and pads
- adequate nutrition and hydration
- protect the skin by the use of additional breathing aids – diapers, special protective dressings – polyurethane film dressing and appropriate skin care products
- documentation of symptoms and changes in body position
Treatment of burn grade II A/B
date of accident: 12/09/2012
end of treatment: 11/10/2012
- The patient from random causes did not seek for help immediately after the accident. This is what the wound looked like 3 days after the accident – 15/09/2012 – size of the wound 65mmx50mm.

- 4 days after the accident the patient went to the doctor (16/09/2012), who applied a antibiotic ointment, and bandaged the wound with a Matovis viscose bandage. The dressing was worn for 12 hours. Over the next eight days the wound was left without any protection.
- The look of the wound after 12 days from the accident – 24/09/2012.

- 13 days after the accident having consulted a specialist treatment using Medisorb specialist dressings was initiated. On 25/09/2012 in the evening 1 tube of Medisorb G was applied on the wound and secured with a Medisorb F secondary dressing. The dressing was left on the wound for 48 hours. The necrosis was hydrated, and the patient began to feel tingling in the wound.
- 15 days after the accident – on 27/09/2012 the dressing was removed, and a Medisorb P was applied on the wound. The edges were covered with an Medisorb F additional dressing, so that the patient could freely take a shower.

- After 7 days from the application – 04/10/2012 – the Medisorb P dressing was removed. The look of the wound.

- 04/10/2012 – the patient applied again Medisorb P on the wound for the next 7 days. Note: In this case even a Medisorb F would have been sufficient.

- 11/10/2012 – removing of the Medisorb P dressing.

- 11/10/2012 a Medisorb F dressing was applied on the wound to protect the delicate tissue against friction. The dressing was removed after 7 days and no other dressing was used.

- 17/12/2012 – the look of the place where the wound was located.

Conclusions:
The burn wound degree IIa / b – the size of the wound 65mmx50mm. For the first 12 days after the accident it was secured just with a bandage, and once an antibiotic ointment was applied. For the next 12 days there was no effect of the treatment. The wound was covered with necrosis.
The treatment with dressings started 13 days after the accident. At first a Medisorb G hydrogel and a Medisorb F film dressing were used. The Medisorb G dressing was to dissolve the necrotic scab and initiate the wound healing process. Medisorb F was only a dressing for the hydrogel. Next the wound with hydrated necrotic tissue was secured with a Medisorb P absorbent dressing that was to absorb the dissolved necrotic tissue. After 7 days of application Medisorb P the wound was already in the epithelisation stage. Finally a Medisorb F was applied just to protect the delicate tissues.
The entire treatment with specialist dressings took 23 days – but the major breakthrough in the wound healing was evident already after 9 days.
For the treatment the following specialist dressings were used:
- 1 x Medisorb G hydrogel dressing 15g
- 3 x Medisorb F film dressings 10cmx12cm
- 2 x Medisorb P polyurethane dressings 10cmx10cm
The cost of the applied dressings is about 40 PLN.
Visible effects of the treatment with specialist dressings occurred after 9 days from their application. After 3 months from the accident there were no signs of the wound. The patient has already forgotten about the accident.
‘Wound’ definition
A wound is damage to the skin and sometimes to deeper underlying tissue and even organs as a result of mechanical, thermal or chemical injury. The wounds caused by mechanical injury include: abrasions, cuts, cracks, stab wounds, bite and surgical wounds. The wounds caused by thermal or chemical injury include: all kinds of thermal, chemical, electrical or radiation burns. There are certain types of wounds – chronic (non-healing) wounds, which are caused by other processes – disease processes. Chronic wounds include: pressure ulcers (trophic ulcers), venous ulcers, neuropathic ulcers and ulcers caused by infections and as a result of radiotherapy or neoplastic processes.
Types of wound healing
1. Slowly healing wounds – healing by granulation
- significant loss of tissue
- the wound cannot be closed by using physical methods
- long healing time
- the treatment is based on the processes of tissue reconstruction – the defect fills in with granulation tissue, on which epidermis appears and forms a scar
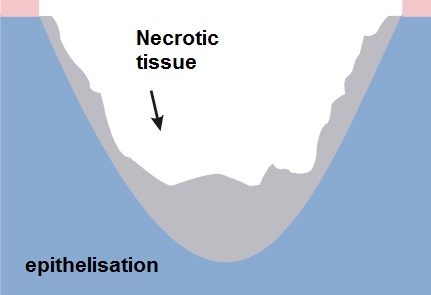
2. Acute wounds – temporary healing by first intention
- surgical or fresh traumatic wounds
- minimum loss of tissue
- edges are joined by seams or using a plaster
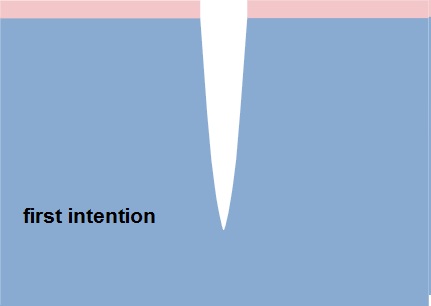
Healing phases
There is no one universal dressing that can be used in each case.
Dressings have different functions: cleansing, absorbent and protective, they often complement each other and none of them alone can meet all the needs of the wound passing through the healing stages:
- inflammation phase (exudate)
- granulation and epithelisation phase (growth)
- maturation phase (reconstruction)
Inflammation phase (exudate)
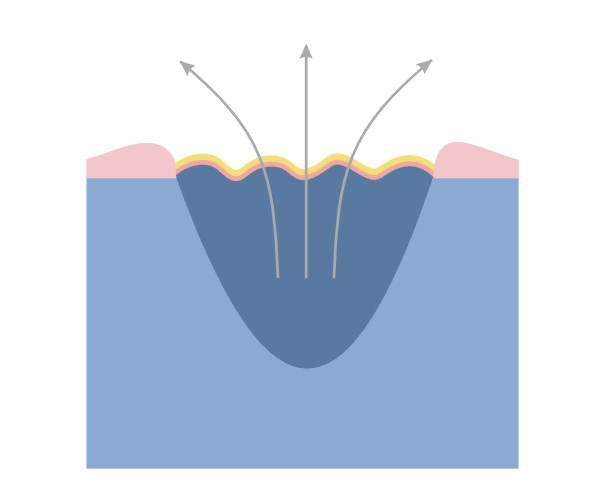
This phase is the body’s response to an injury. Due to circulatory disorders, enlargement and increased permeability of capillaries oedema occurs, accompanied by exudate.
Functions of the dressing in the inflammation phase:
- stemming the bleeding
- facilitating natural debridement
- absorbing excess exudate
- preventing re-infection
Granulation and epithelising phase (growth)
Granulation – the change from the inflammatory phase into the proliferative phase, which is controlled by macrophages and other cells. Macrophages stimulate fibroblast growth.
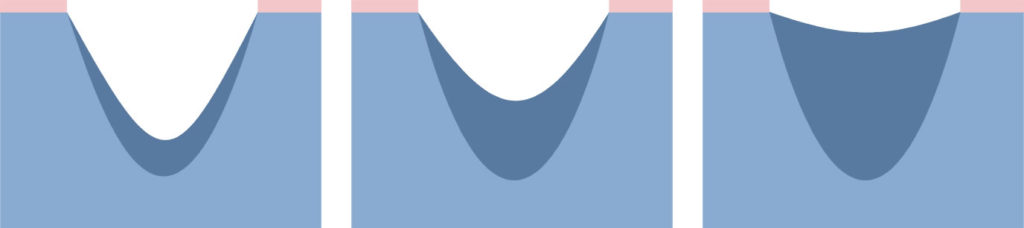
Fibroblasts fill the space that is left after the lost tissue with granulation tissue.
Narrowing of the wound – many fibroblasts is transformed into myofibroblasts. The network of connected myofibroblasts pulls the edges of the wound together (0.6-0.7 mm/day).
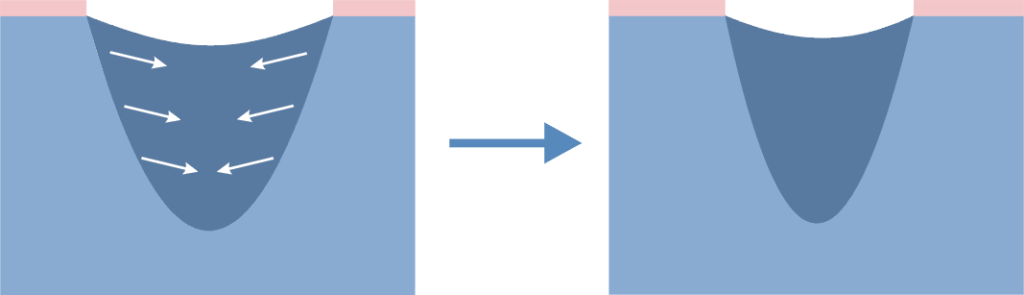
Narrowing of the wound makes the scar smaller than the original wound.
Epithelisation – new epidermis, which is needed for the complete closure of the wound. Epidermal cells migrating from the edges of the wound cover the granulation tissue and create new skin.
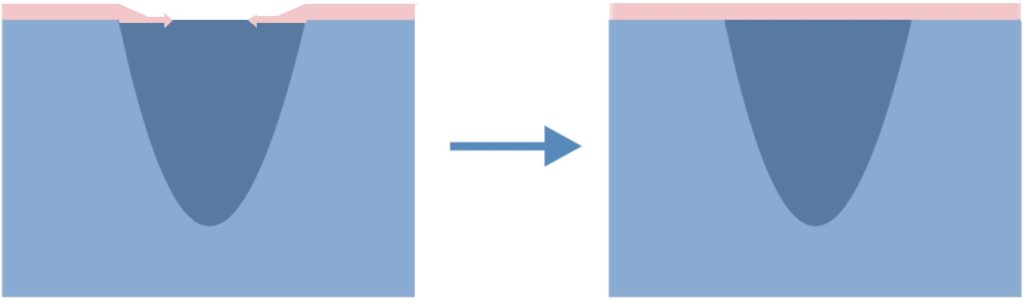
Functions of the dressing in the growth phase:
Granulation
- maintaining moist environment
- absorbing excess exudate
- protecting against mechanical injury
- preventing re-infection
Epithelisation
- maintain a moist environment
- protecting delicate epidermis during dressing changes
Maturation phase
Maturation – slow reorganisation of microscopic structure of scar tissue; the remodelling results in improving the strength of the scar, its reduction and smoothing.
This stage can last for months or even years.
In the treatment of abnormal scarring are the following items are used:
- topical silicone dressings
- compression bandages or special compression garments
- surgery, corticosteroid therapy, laser and cryosurgery
Functions of the dressing in the maturation phase:
- smoothing the scar
- whitening the scar
- reducing the scar
What is wound exudate?
Wound exudate is a particular fluid called in the past “nature balm” appears in the first stage of wound healing, immediately after an injury.
The exudate contains a variety of ingredients including nutrients for actively metabolising cells:
- very few red blood cells
- up to 6 times more white blood cells than in the blood
- less glucose, but the same amount of minerals as the blood
- proteins – among which there are enzymes important for the wound healing processes; the released enzymes cleanse the wound and remove damaged tissues
In a normally healing wound the amount of exudate decreases with time. In a wound, in which the healing process is disturbed, the amount of exudate is not reduced in time and its management can be a big challenge for dressings.
NOTE: to maintain the best possible conditions for wound healing the optimal amount of wound exudate is needed, namely a so-called moist wound healing environment.
Too much exudate and its absence can slow down the healing process. Therefore, it is important to choose an appropriate dressing to the amount of wound exudate. In wounds dry without exudate the dressing should moisten, and in wounds with too much exudate preferably the dressing should absorb its excess.
NOTE: The change in colour, odour and exudate density may indicate a change in the wound or the appearance of inflammation / infection – it is a signal that the wound should be examined and assessed by a specialist.
Dressing type vs. indication for its use in wounds with various exudate amount
| Dressing type | Level of exudate | ||||
| none | low | medium | high | medium/high | |
| challenge for the dressing | hydrate the wound | maintain a moist environment | absorb the excess of exudate | absorb the excess of exudate | drainage of excess exudate to the secondary dressing |
| hydrogel | √ | √ | |||
| polyurethane film | √ | ||||
| hydrocolloid | √ | √ | |||
| polyurethane foam | √ | √ | |||
| alginate | √ | √ | |||
| resorbable | √ | ||||
Wound treatment models
The traditional wound healing model
Through the centuries chronic wounds were treated using a variety of materials that were to dry the wound.
The traditional wound treatment system based on the use of absorbent dressings made of gauze which:
- ensured the absorption of excess exudate
BUT
- failed to protect the wound against drying out and cooling down, which slowed down the rate of healing
- did not constitute adequate protection against external factors, which could lead to frequent wound infections
- adhered to the wound, which damaged the new tissue and caused pain to the patient during dressing changes
- with limited absorptive capacity compelled to frequent dressing change
Dry wound healing is still the most desirable but for acute wounds healing by first intention.
The modern wound healing model
Since the publication of research by George Winter, it became clear that wounds heal much more quickly if the healing process is carried out in humid conditions in which the optimal amount of exudate is maintained on the surface of the wound. In view of the conditions under which the treatment process takes place, the concept was called A MOIST WOUND HEALING.
According to this concept, the treatment deals with closing the wound with a special dressing which:
- maintains the required level of moisture on the wound surface to create an optimal healing environment
- initiates autolytic cleansing, which leads to faster debridement and to start the healing process
- thermally isolates the wound which keeps the temperature at a constant level and accelerates the healing process
- provides long-term absorption of excess exudate, reducing the number of dressing changes
- does not adhere to the wound thanks to which dressing change is safe for young tissues and painless for the patient
- is water-resistant and protects the wound against external environment, which minimises the risk of infection
Features of a perfect dressing
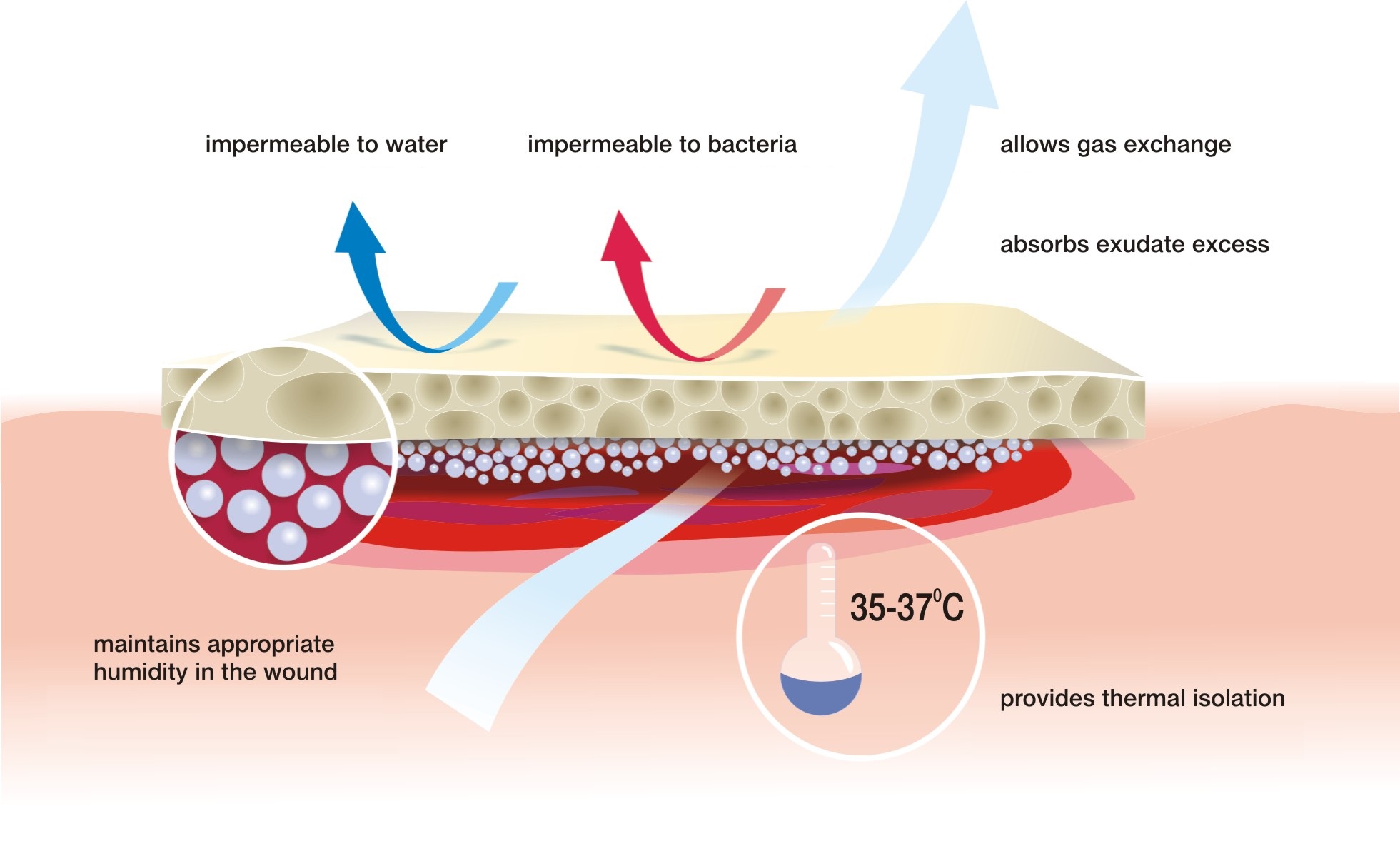
Moist wound healing is most appropriate for hard-to-heal wounds but it can be also used for the treatment of usual cuts, abrasions or scratches.
Hanna Szymkiewicz
European Centre for Long-Term Care
A wound is a skin break, which may extend to deeper tissues and organs. The cause of the wound can be internal and external factors associated with physiological disturbances. The breadth and depth of the wound depends on the causative agent, its strength and areas it affected.

Division of wounds due to the causative agent:
>> exogenous factors:
- mechanical (cut, stab, mashed, gunshot wounds)
- thermal (burns, frostbites)
- chemical (chemical burns)
- electrical (burns)
>> endogenous factors
- ulcers (leg ulcers, pressure sores, diabetic foot) – e.g. impaired circulation
Division of wounds due to the healing time:
- sharp – less than 8 weeks
- chronic – more than 8 weeks
Division of wounds due to the way healing:
- acute wounds – cuts, surgical wounds with even edges and in which there is no substantial loss of tissue. Such wounds are closed with sutures, staples or a dressing, and the wound is healed by first intention and lasts about 6-7 days. It is the most preferred way of healing, and is referred to as primary healing.
- chronic wound – wounds where there is a significant loss of tissue and / or infection. In this case, it is not possible to bring the wound edges together. This type of wound healing by granulation (secondary intention) – the inflammatory phase is followed by proliferative phase, in which the tissue loss is filled with granulation tissue. This process is called secondary healing.
Secondary healing
Secondary wound healing concerns chronic wounds – including bedsores, ulcers, and complicated wounds caused by exogenous factors, such as complex surgical wounds. There are three phases in this healing:
- inflammatory phase (purification)
- proliferation (granulation)
- maturation
The inflammatory phase is characterised by an inflammatory reaction and pain. The body is trying to destroy the bacteria that get into the wound after the discontinuation of the skin. Exudate appears. The dead tissues are excreted out or absorbed by the organism. The wound gets covered with blood clot, which protects it from germs.
In the proliferation phase the exudate is reduced, vessels get narrower, and this is followed by granulation – filling the tissue loss and epithelialisation – the wound is covered with new epidermis.
In the maturation phase the rebuilding process of the newly healed wound takes place to get the strength similar to the intact skin.
The process of healing and its duration depends on many different factors: the general condition of the patient: the age, nutritional status and co-existing diseases; the type of the injury, its location, its closure way, its cleanliness and the time that has passes since the injury to its dressing.