
No search results
Causes
The cause of pressure ulcers (also called bedsores, decubitus ulcers or pressure sores) is tissue ischemia due to the prolonged pressure evoked on veins and arteries.
The risk of pressure ulcers depends on the duration of the pressure – the longer the pressure is present or the greater the force, the greater the possibility of developing bedsores.
In healthy people prolonged pressure causes pain forced to change position.
Unconscious and immobile people are not able to relieve the pressure automatically and to improve the blood circulation, thus they belong to the group of people at increased risk of pressure ulcer development.
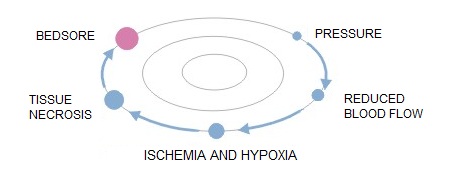
Pathomechanism of developing bedsores:
- simple pressure i.e. the pressure exerted on the soft tissue on one side by the bone, and on the other by a hard surface
- rubbing the patient’s body surface over bed linen e.g. when using improper technique for changing positions
- lateral tensile forces, which act directly on the patient’s body
Risk group
The risk of developing pressure ulcers should be considered in all patients with long-term reduction of capacity for self-movement, which spend most of their time in bed or in a wheelchair.
Factors that increase the risk of pressure ulcer development are:
- age
- weight
- nutritional status
- sphincter function of the urethra and the anus
- state of consciousness
- diabetes, atherosclerosis
- steroid therapy
Symptoms
Pressure ulcers are classified according to the severity of the symptoms into 4 or 5 degrees. And hence:
- Stage I: intact skin with non-blanchable redness of a localised area usually over a bony prominence. The area may be painful, firm, soft, warmer or cooler as compared to adjacent tissue. Microcirculation is not damaged yet.
- Stage II: partial thickness loss of dermis presenting as a shallow open ulcer with a red pink wound bed, without slough. Presents as a shiny or dry shallow ulcer without slough or bruising.

- Stage III: abrasions, cracking skin and full-thickness skin damage to the border of the subcutaneous tissue, blisters, the wound edges are well marked out, surrounded by edema and erythema

- Stage IV: the damage extends towards the subcutaneous fatty tissue; the ulceration can be free from infection and necrosis and covered with clear granulation tissue, but the necrosis may also affect the fatty tissue and the surrounding skin layers. The bottom may be covered with black necrosis.
- Stage V: the presence of advanced necrosis, which extends towards the fascia and muscles; the damage can also affect joints and bones – unpleasant odour and profuse pus-necrotic discharge; in the wound there are pieces black dead tissue and black necrosis

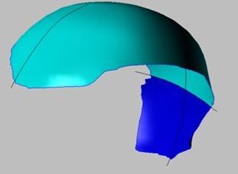
Location
Bedsores occur in places where the distance between bone prominence and the skin surface is the smallest i.e. in contact point of the skin and the ground, where the pressure is the highest. Most pressure ulcers are formed around the aitchbone, coccyx, buttocks, on the heels or the hips.
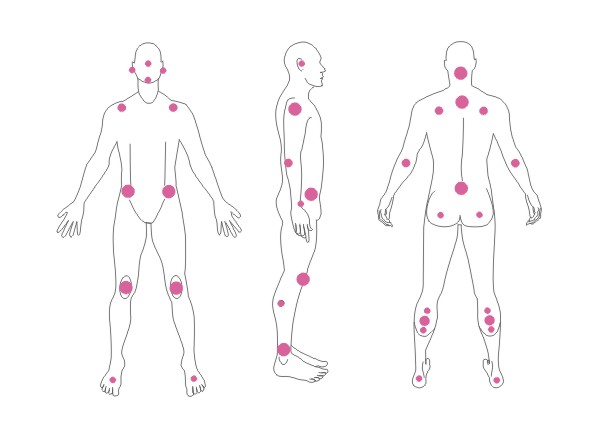
The above figures present the point of contact of the skin with the surface at various positions of the patient laying on the bed.
Where to seek help and advice
Of course, in the first place consult the general practitioner.
The treatment of pressure ulcers is the responsibility of a doctor and a nurse who has completed a specialist course in the treatment of chronic wounds. The competences of nurses are limited to the treatment of pressure 1 to 3 degree sores.
Sometimes the condition of the wound requires surgical debridement and then the GP directs us to a specialist surgeon.
The treatment of pressure ulcers is tough and long-lasting so to make it the least expensive and effective it must be based on genuine and systematic cooperation of the doctor and the patient, and must be combined with an intensive, professional care.
Treatment
First of all the treatment should be conducted under the supervision of a doctor or a nurse.
Bedsores are treated locally i.e. the wound is to be secured with dressings appropriate.
A very important part of treatment is also appropriate patient care, which include:
- position changing – the patient should not lie on the bedsore
- placing patient on a pressure relief mattress
- protecting sore places with special anti-bedsore discs and stands
- adequate nutrition and hydration of the patient
- controlling comorbidities
The most effective form of treatment is the use of specially designed wound dressings for this purpose, the so-called specialised or advanced dressings that create a moist wound healing environment.
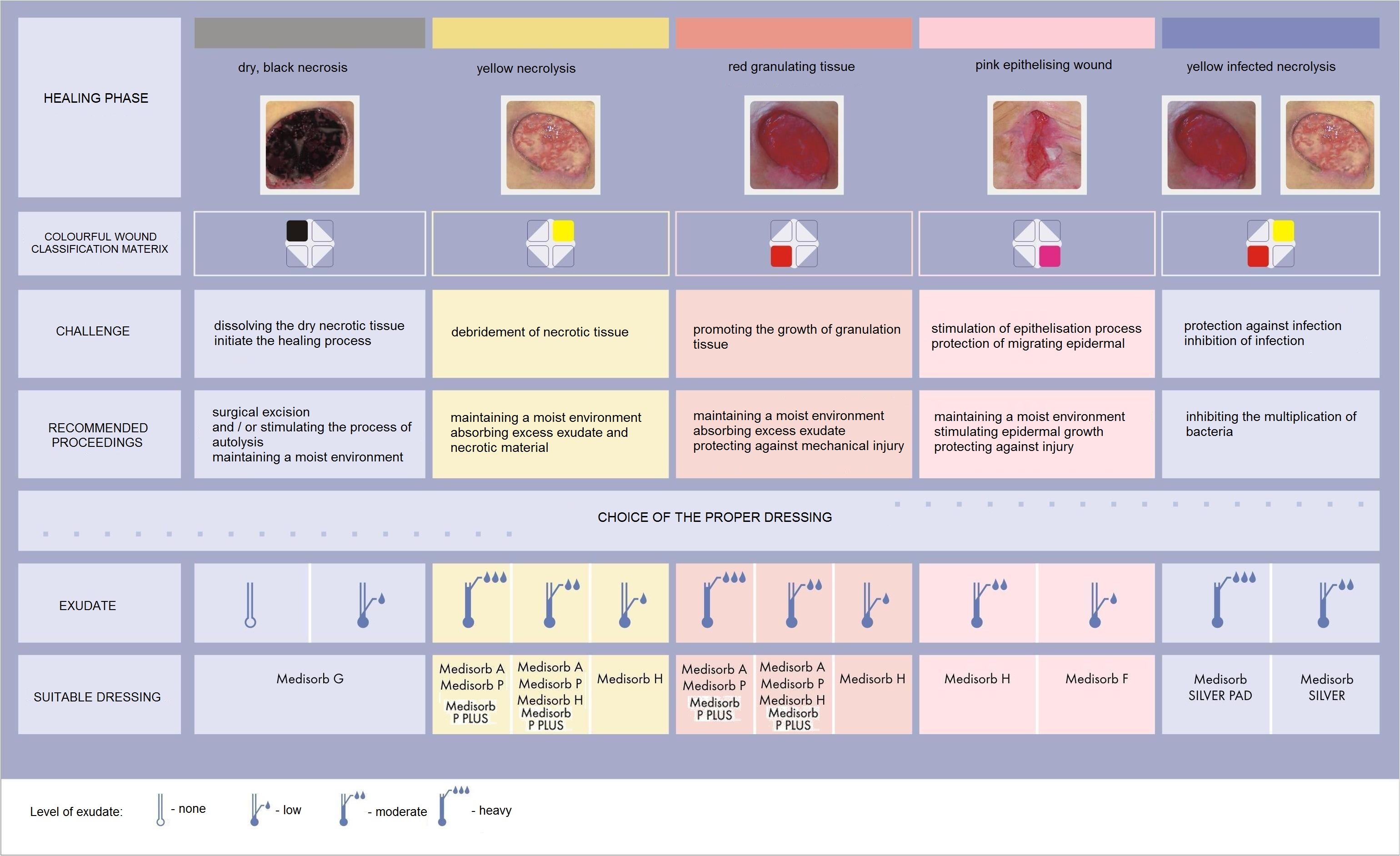
Choosing the right, effective dressing it must be based on a correct diagnosis of the processes occurring in the wound. To make it easier, you can use the wound colour classification matrix, which is based on the observation of the phenomena that take place in different phases of healing.
Wound colour classification matrix:

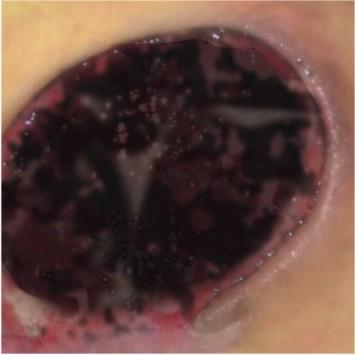
Black wounds

Wounds with black necrosis require:
- maintaining a moist environment
- removal of necrotic tissue in order to initiate the healing process
The healing process will not occur under thick layers of necrotic tissue; to begin it first the necrosis needs to be removed. We have a choice of two basic ways to get rid of the necrosis from the wound bed:
- surgical debridement – the mechanical removal of necrotic tissue to expose healthy skin structures for initiating the process of wound healing
- application of interactive dressings – involves the application of dressing on a wound, which stimulates the autolysis process i.e. the natural wound cleansing by the body. In this case the necrosis decomposition is made by enzymes produced by the damaged wound cells.
Recommended dressings for black wounds:
- Medisorb G – hydrogel dressing
Yellow wounds

Wounds with yellow, colliquative necrotic tissue require:
- maintaining a moist environment
- absorbing excess exudate, along with the remnants of necrotic material
Wounds with colliquative necrosis are characterised by an increased exuding level. The necrosis on the bottom of the wound is liquid. Such wounds provide an ideal environment for the growth of microorganisms, and therefore they are often infected. The tasks for the dressing in this case is the absorption of exudate and necrotic material, liquefaction of too dry and too dense necrosis, protection against drying out and against secondary injuries.
Recommended dressings for yellow wounds (depending on the exudate level and the depth of the wound):
Medisorb A – alginate dressing – heavy or moderate exuding wounds; superficial and deep wounds
Medisorb P – absorbent dressing – heavy or moderate exuding wounds; superficial wounds
Medisorb H – hydrocolloid dressing – moderate and low exuding wounds; superficial wounds
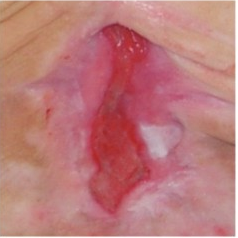
Red wounds

Red wounds with visible granulation tissue required:
- maintaining a moist environment
- protecting against secondary infections
- controlling the exudate level
Apart from maintaining a moist environment, these wounds also require protection against possible mechanical injuries. This is particularly important since a well-vascularised granulation tissue is susceptible to injuries which delay the healing process and can be the source of infection. Another important factor is to maintain the proper temperature (close to body temperature), so that new cells can grow at optimum speed.
Recommended dressings for red wounds (depending on the exudate level and the depth of the wound):
- Medisorb A – alginate dressing – heavy or moderate exuding wounds; superficial and deep wounds
- Medisorb P – absorbent dressing – heavy or moderate exuding wounds; superficial wounds
- Medisorb H – hydrocolloid dressing – moderate and low exuding wounds; superficial wounds
Pink wounds

Pink epithelising wounds require:
- maintaining a moist environment
- protecting sensitive tissues
When the wound begins to cover with epidermis it needs to be protected against drying out, friction and other factors that could damage the newly formed tissue.
Recommended dressings for pink wounds (depending on the exudate level and the depth of the wound):
- Medisorb H – hydrocolloid dressing – moderate and low exuding wounds; superficial wounds
- Medisorb F – film dressing – low exuding wounds
The analysis of wound healing phases shows that wounds being at various stages of healing, require some other conditions for the process to run smoothly. It is important to remember that in addition to various healing stages, the wounds are also varied because of the size, depth, presence of necrotic tissue and exudate level. All these features result in the fact that each wound requires the selection of the right kind of dressing, sometimes even a few dressings that will change during the healing process.
The following table presents factors that may slow down the healing process.
Table: Factors slowing down the wound healing process
| slowing down factor | why | optimum conditions | how does it work in optimum conditions |
| dry environment | moist environment | appropriate level of wound exudate: allows activation of natural wound debridement; accelerates granulation; provides quick and correct course of epithelisation | |
| necrotic tissues | wound healing is possible only after the removal of dead tissues; the necrosis may be a substrate for the development of infection | curgical / autolytic wound cleansing | cleansed the wound enable the begin of the granulation phase |
| infection | all mechanisms in the wound tend to fight the intruder; the healing process is hampered | fight infection | cleansed the wound enable the begin of the wound healing process |
Prevention
Basic rules:
- systematic change of body position every two hours and reduce pressure in places at risk, through the use of special pressure relief mattresses and pads
- adequate nutrition and hydration
- protect the skin by the use of additional breathing aids – diapers, special protective dressings – polyurethane film dressing and appropriate skin care products
- documentation of symptoms and changes in body position
Causes
Burns are the result of the action of high temperature, chemical corrosion or current. The most common causes of burns is the heat, which may come from boiling water, steam, hot liquids or semi-liquids like fat or paraffin, as well as burns caused by household appliances.
In electrical burns the main damaging agent is high voltage passing through tissues and heating them. Chemical burns are usually caused by the action of acids or usual alkalis. Regardless of the genesis, burns are specific types of injuries and can cause serious complications for the patient.
Risk group
The risk of burns should be considered in all people, but most of all:
- children at the age 2 to 4 years
- adults working in hazardous conditions (miners, steelworkers, firefighters, welders, etc.)
Symptoms
The main factor determining the type of burn is its depth, by which we distinguish the following types of burns:
- First degree (superficial) – affects only superficial layers of the epidermis. The main symptoms of the damage is vivid red erythema and pain. The wound usually heals without complications and leaves no scars.
- Second degree A (superficial partial thickness) – affects almost the entire layer of the epidermis and superficial dermis. Wounds are usually vivid red, very painful, and are characterised by blisters. 2nd degree burn injury may leave slight discoloration, and sometimes scars.
- Second degree B (deep partial thickness) – the epidermis and deeper dermis layers are destroyed. In this type of injury superficial epidermal and skin necrosis is observed. This type of injury is very painful, blistering free, pale or pink, grey, brick red and even black. Moreover, they can leave negative hypertrophic scars.
- Third degree (full thickness) – extends through entire dermis. The wounds usually are pale brown, brown, pale yellow or red. They leave scars and can lead even to amputation.
- Fourth degree – extends through the entire skin, and into underlying fat, muscles, tendons, bones, joints.
Location
Burns occur in places of body contact with thermal factors.

Typically this affects:
- trunk
- upper limbs
- lower limbs
Where to seek help and advice
First degree burns
can be treated at home, and if there is in the progress in the treatment or complications appear consult your GP
Second and third degree burns
a hydrogel dressing should be applied as soon as possible, e.g. Medisorb G and immediately consult your doctor or contact the emergency station
Fourth degree burns
immediately contact the emergency station or the nearest hospital
Treatment
Depending on the burn degree the treatment is carried out in different ways.
First degree burns – affect only the epithelium. The place that was burned is red, slightly swollen and dry. The victim feels strong burning sensation. Quick application of a hydrogel dressing such Medisorb G allows for quick healing of the wound.
Second degree burns – damage the dermis. It becomes red, and on the surface there are blisters formed that fill with fluid tissue. Second degree burns are very painful. Similarly to the first degree burns rapid response using hydrogel dressings such Medisorb G allows for quick healing. If the burn is extensive, it requires hospitalisation.
Three and four degree burns – affect the tissue located under the skin. Also the connective tissue, blood vessels, muscles, and nerves can get damaged. The skin may take on waxy appearance, whitish or charred colour. The victim may not feel any pain because nerve endings have been destroyed. This type of burns require immediate medical help, sometimes even a skin graft or recovery in the hyperbaric chamber might be needed.
A common complication after recovering from burn wounds are hypertrophic scars and joint contractures. Their long recovery should be carried out using pressotherapy or rehabilitation of scars by means of compression products such as Codopress® combined with silicone dressings Codosil® ADHESIVE.
Prevention
Past statistics show that each year different types of burns affect about 1% of our population. According to these data, the number of Poles affected by various types of burns is up to 400 000 patients per year. Burns are very often associated with the type of activity of patients, as well as with age. Approximately 50-80% of burn victims are mainly children at the age 2 to 4 years.
Prevention of burns should primarily focus on the preparation of the house where the little man will feel safe:
- Never leave a young child alone.
- Avoid placing hot drinks, soups or dishes taken out directly from the oven on a table.
- In homes with young children – especially those crawling ones – there should be no tablecloths – pulling by the tablecloth a child pull down everything what stands on the table.
- Do not leave a turned on iron in the room, where a child is present; a turned off iron must cool down and also be out of reach of children.
- When cooking meals try to do use gas jets at the wall – those being away from your baby; you can use a special shield that prevents a child from touching a hot pot or pull it down.
- Owners of ceramic cooking plates should be aware that a turned off plate does not allow the child to notice the danger, and touching it before it cooled down can result in serious burns.
To sum up – parents should not leave their children unattended!
Maria T. Szewczyk, Ph. D.
Department of Surgical Nursing, Ludwik Rydygier Collegium Medicum in Bydgoszcz, Nicolaus Copernicus University in Toruń
In the treatment of ulcers, especially of their advanced form, omnidirectional and interdisciplinary care of the patient is required. Venous ulcers are chronic wounds, where the healing process is difficult and lengthy, and requires the effort of many measures. (…)
Chronic venous insufficiency and venous ulcers
In about 80% of cases the cause of leg ulcers is chronic venous insufficiency. Venous ulcers are the final and most serious complication. In the treatment of ulcers, especially of their advanced form, omnidirectional and interdisciplinary care of the patient is required. Venous ulcers are chronic wounds, where the healing process is difficult and lengthy, and requires the effort of many measures. Extensive and ongoing for years wounds often lead to movement limitation in the ankle joint, foot deformation and permanent disability (Photo 1, 2, 3, 4).

(archive of the author)

(archive of the author)

(archive of the author)

(archive of the author)
The first step is the diagnostic and ultrasound examination of venous vessels, and then topical and causal treatment. Etiopathogenesis, in which the main role plays venous hypertension, requires at first elimination or reduction of causative factors. The cause of ulcers are in fact circulatory disorder leading to the venous hypertension in the lower limbs. These relate to pathological anatomical and physiological changes occurring in several successive stages. It begins with overload and baggy or fusiform enlargement of the vascular system in the form of varicose veins. Accompanying changes include: a decrease of flexibility and patency of blood vessel walls, and valvular regurgitation, venous blood reflex and (or) occlusion of the deep venous system (by e.g. deep vein thrombosis). Long-lasting high hydrostatic pressure eventually leads to an increase in vascular patency and transition – first of exudate and also of cellular components. In the so-called gaiter area of the leg (the lower half of the leg above the ankle and around the ankle) trophic changes occur, initially only in the form of over-pigmentation and discolouration, and later also in the form of inflammation, fibrosis and thinning of the skin tissue. On the surface of these changes ulceration can be developed. The immediate cause of the injury can be not only the changes in the skin nutrition, but also spontaneous rupture of varicose veins, or even a slight mechanical shock.
The gold standard of conservative treatment of venous ulcers is compression therapy followed by wound cleansing and active moist or biological dressings.
Compression therapy
In the conservative treatment a vital role plays compression therapy, which deals with individually chosen compression dressings. It can be bandages (band) with compatible compression degree as well as ready products in the form of knee-length, short and long stockings and tights. The compression therapy using the bandages depends inter alia on the material from which they are made and the method of bandaging the limb. The use of the compression greatly reduces venous hypertension in the superficial system, improves the efficiency of the muscle pump, reduces venous stasis and restores proper hydrostatic conditions for the outflow of blood from the vessels. The compression will be effective if the degree of compression will be applied depending on the severity of chronic venous insufficiency i.e. it will depend on the superficial, perforator and deep vein system. To measure the interfacial pressure of the compression a Kikuhime device is used. With the help of this apparatus we can provide the required pressure. (Photo 5)

(archive of the author)
Similar effects can be brought by a massage – both sequential pneumatic massage (Photo 6) and manual massage reducing the oedema and improving the return of venous blood towards the heart.

(archive of the author)
Before the use of compression the state of the peripheral circulation must be checked. The use of compression therapy in a patient with impaired blood flow can result in severity of ischemia, skin necrosis, and even limb amputation. Therefore, before applying the compression therapy is necessary to perform Doppler imaging and marking the Ankle Brachial Index (Photo 7).

(archive of the author)
Topical proceedings
The topical proceedings parallel with the compression therapy includes: necrosis removal, wound debridement, moist wound healing, care of the skin around the wound.
Contaminations, superficial necrosis reaching the dermis can be removed in a conservative way, e.g. mechanical, enzymatic, autolytic, and in a surgical way. However, necrotic tissues, including subcutaneous layers require a surgical intervention by removal of the changed tissues with a scalpel and scissors. You can also include the VAC system (vacuum-assisted wound closure) as a non-invasive active therapy to promote healing in difficult wounds that fail to respond to established treatment modalities. The method of necrosis removal is determined by the location and depth of the ulcer, the exudate amount in the wound and the patient’s general condition. Of great importance in the selection of the treatment method is the nature and extent of necrosis structures. The mechanical wound debridement, as well as the surgical debridement of wound edges give immediate effect to remove necrotic elements. The autolytic debridement is a natural process that occurs spontaneously in a properly healing wound. It is the effect of proteolytic enzyme and phagocyte activity , which can be both initiated and supported by the maintenance of moist environment at the bottom of the wound. Low severity of these processes in the debridement phase might require to use ready proteolytic enzymes and to introduce enzymatic debridement. Wound cleaning and removal of the necrosis reduces the risk of infection and the development of a local infection. The purpose of this treatment is to prepare the wound to further proliferative processes and stimulation of these processes to maintain optimal healing conditions. Please note that venous ulcers are heavily exposed to the risk of infection. It can be caused by different types of microorganisms (viruses, bacteria and fungi), but the most common etiological agent are bacteria, including staphylococci, streptococci, Escherichia coli and Pseudomonas. Proliferating in the wound, the bacteria secrete its own metabolites and toxins, destroying migrating fibroblasts and budding vessels, and limiting the healing progress. An uncontrolled infection can spread deep inside the wound, infiltrate adjacent tissues, and even lead to the development of sepsis.
The risk of infection and the development of infection can be additionally reduced by flushing the wound bed with antiseptic solution. Its concentration should not only have a bactericidal or bacteriostatic effect, but also should be safe for healthy tissue and does not cause cytotoxic effects or inhibit the healing. Only the preparation meeting the above criteria can be safely applied directly on the wound surface (e.g. Octenisept containing a mixture of octenidyne dihydrochloride and phenoxyethanol safe for skin and mucous membranes). In justified cases general antibiotics are used, which should not be used topically. To support the natural debridement and recovery processes, on a clean wound a special active dressing maintaining moist wound healing environment should be applied.
Moist wound healing
Features of the “ideal” dressing, developed on the basis of Winter analysis (1962) and his successors are satisfied by so-called new generation dressing. They maintain adequate moisture wound environment, which prevents the scab formation and drying out of the ulcer surface. A moist wound heals twice as fast and in a more structured way, because the moist environment stimulates both cell proliferation and the migration of new cells, ensuring their optimal differentiation and neovascularisation.
Features of a dressing supporting the natural healing processes were defined in 1991 by Turner et al:
- maintains a moist environment in the wound bed,
- has high absorption capacity, regulates the excess of exudate,
- does not adhere to the wound surface, enables painless and atraumatic change,
- protects the wound against bacteria and contamination,
- is non-toxic and non-allergenic,
- maintains the correct wound temperature similar to the body temperature,
- facilitates the healing process at all wound healing stages.
The new generation dressings fulfilling the listed criteria are produced in several groups, differing in the design and application. They are designed for different types of wounds, depending on their etiology, the healing phase, the depth of tissue damage, the nature of the exudate and the presence of an infection.
The dressings have different properties to keep the exudate, whose secretion varies during the particular wound healing phases. Apart from the outer protection and moisture content control the dressing has to fulfil other important task at every stage of venous ulcers healing.
Skin care
The management of chronic venous insufficiency in states with weak skin barrier function requires particularly attentive care and concentration of efforts aimed at conditioning and regeneration of the natural protective barrier of the epidermis. One of the major care actions taken in concern of the integrity of the skin is to maintain the cleanliness of the body, including the limbs. Cleaning agents used for personal hygiene should be properly chosen and correctly applied, especially when it comes to this group of patients. Detergents are designed to remove and reduce the number of contaminations and microorganisms residing on the surface of the body, if possible without damaging the skin protective barrier. Since the lipid coat has the properties of “binding” impurities, and water alone is not able to overcome them, the washing agent needs to contain surfactants. It is recommended to use agents that are delicate, have a pH of 5.5 or liquid agents containing a substance modifying the acidity of the product (for example: phosphoric acid, citric acid, sodium hydroxide, triethanolamine), and enriched with physiological lipids, ceramides, and moisturising agents, which at least partially allow to compensate for the lipid loss caused by the action of the detergent.

(archive of the author)
After thorough cleaning of the skin it is advised to apply agents supporting the regeneration and increasing the moisture level of the skin. This can be obtained thanks to biologically inert substances supporting the treatment and skin care of the, so-called emollients. Due to moisturising properties, they increase the water content of the stratum corneum and improve the biophysical properties of the epidermis (Photo 8). The emollients are available in form of creams, lotions, ointments and emulsions of different consistency, serving the same purpose – moisturising and / or oiling the dry skin. Creams and ointments usually need to be applied thicker. Agents of lighter consistency, such as lotions, make it possible apply thin film. Agents applied on sensitive skin should not contain alcohol, metals, fragrances, or talc. In specific situations they should contain only water-based hydrophilic ingredients. Distributed on the skin they are easily absorbed, and after washing do not leave unwanted residues.
Literature:
- Benbow M, Burg G, Comacho Martinez F, et al. Guidelines for the outpatient treatment of chronic wound and burn. Blackwell Science, Berlin-Vienna 1999, 12-21.
- Szewczyk MT, Jawień A.: Chosen aspects of conservative treatment of venous ulcers. Part I: Compression therapy. Progress Dermatol. Alergol. 2005, XXII, 3: 133-140.
- Blair S, Wright D, Blachkouse C, et al. Sustained compression and healing of chronic venous Ulcers. Br Med J 1998, 298: 1159-1161.
- Ciecierski M, Jawień A. Clinical picture of chronic venous insufficiency. Medical guide 2004, 8 (68): 36-48.
- Hess CT. When to use hydrocolloid dressing. Nursing 1999; 29.11: 20-23.
- Szewczyk MT, Jawień A, Piotrowicz R. Treatment of venous ulcers. Medical guide 2004, 8 (68): 66-71.
- Szewczyk MT, Jawień A, Piotrowicz R. The use of compression therapy in venous diseases. Medical guide 2004, 8 (68): 58-64.
- Jawień A. Szewczyk MT. (red) Venous leg ulcers. Ed. Your Health. 2005.
- Jawień A. Szewczyk MT. (red) Clinical and nursing aspects of care for patients with venous ulcers. Termedia 2008.
- Szewczyk MT., Mościcka P., Cwajda J. et al Evaluation of the effectiveness of new polyurethane foam dressing in the treatment of heavily exudative venous Ulcers. Acta Angiol. 2007 T.13, 2: 85-93.
- Placek W. Role of substrates and emollients in the prevention and restoration of the epidermal barrier. Aesthetic Dermatology 1999, 4: 174-178.
- Korinko A. Yurick A. Maintaining skin integrity Am J Nurs 1997 (2): 40-44.
- Wojnowska D., Chodorowska G., Juszkiewicz-Borowiec M. Dry skin – pathogenesis, clinic and treatment. Advances in Dermatology and Allergology, 2003, XX, 2: 98-105.
- Szewczyk MT, Jawień A. Recommendations of specialised nursing care of patients with venous leg ulcers. Surgical and Vascular Nursing 2007, 3 (1): 95-129.
Treatment of burn grade II A/B
date of accident: 12/09/2012
end of treatment: 11/10/2012
- The patient from random causes did not seek for help immediately after the accident. This is what the wound looked like 3 days after the accident – 15/09/2012 – size of the wound 65mmx50mm.

- 4 days after the accident the patient went to the doctor (16/09/2012), who applied a antibiotic ointment, and bandaged the wound with a Matovis viscose bandage. The dressing was worn for 12 hours. Over the next eight days the wound was left without any protection.
- The look of the wound after 12 days from the accident – 24/09/2012.

- 13 days after the accident having consulted a specialist treatment using Medisorb specialist dressings was initiated. On 25/09/2012 in the evening 1 tube of Medisorb G was applied on the wound and secured with a Medisorb F secondary dressing. The dressing was left on the wound for 48 hours. The necrosis was hydrated, and the patient began to feel tingling in the wound.
- 15 days after the accident – on 27/09/2012 the dressing was removed, and a Medisorb P was applied on the wound. The edges were covered with an Medisorb F additional dressing, so that the patient could freely take a shower.

- After 7 days from the application – 04/10/2012 – the Medisorb P dressing was removed. The look of the wound.

- 04/10/2012 – the patient applied again Medisorb P on the wound for the next 7 days. Note: In this case even a Medisorb F would have been sufficient.

- 11/10/2012 – removing of the Medisorb P dressing.

- 11/10/2012 a Medisorb F dressing was applied on the wound to protect the delicate tissue against friction. The dressing was removed after 7 days and no other dressing was used.

- 17/12/2012 – the look of the place where the wound was located.

Conclusions:
The burn wound degree IIa / b – the size of the wound 65mmx50mm. For the first 12 days after the accident it was secured just with a bandage, and once an antibiotic ointment was applied. For the next 12 days there was no effect of the treatment. The wound was covered with necrosis.
The treatment with dressings started 13 days after the accident. At first a Medisorb G hydrogel and a Medisorb F film dressing were used. The Medisorb G dressing was to dissolve the necrotic scab and initiate the wound healing process. Medisorb F was only a dressing for the hydrogel. Next the wound with hydrated necrotic tissue was secured with a Medisorb P absorbent dressing that was to absorb the dissolved necrotic tissue. After 7 days of application Medisorb P the wound was already in the epithelisation stage. Finally a Medisorb F was applied just to protect the delicate tissues.
The entire treatment with specialist dressings took 23 days – but the major breakthrough in the wound healing was evident already after 9 days.
For the treatment the following specialist dressings were used:
- 1 x Medisorb G hydrogel dressing 15g
- 3 x Medisorb F film dressings 10cmx12cm
- 2 x Medisorb P polyurethane dressings 10cmx10cm
The cost of the applied dressings is about 40 PLN.
Visible effects of the treatment with specialist dressings occurred after 9 days from their application. After 3 months from the accident there were no signs of the wound. The patient has already forgotten about the accident.
Violeta Senavaitienė
Matopat Representative – Lithuania
22/02/2013
1. Place – Panevezys (Lithuania)

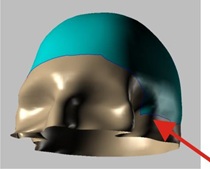
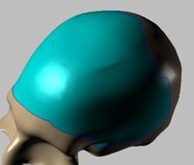
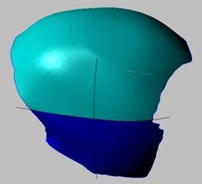
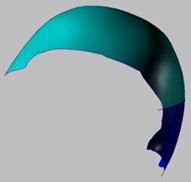
On February 14, 2013, a Codubix® CT (individual skull bone prosthesis) was implanted in the State Hospital in Panevezys.
2. Situation and circumstances
In September 2012 I prepared a presentation for neurosurgeons about Codubix® products. I introduced all the possibilities and advantages.
About two months later I got a call from the hospital. A patient appeared who needed a Codubix® CT individual prosthesis.
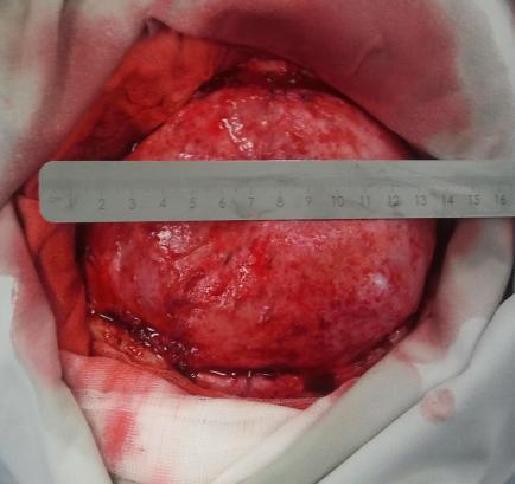
The patient had most of the skull bone removed after a stroke with a large swelling of the brain. It was the only way to save her life. After the operation the patient was fully conscious and active. But there was one problem – how and with what to cover the missing part of the skull.
The product, which was available in the hospital was not sufficient to help with so a damage. It was decided to prepare an individual prosthesis.
3. Actions till the operation
On 5/11/2012 under my leadership all the necessary computer images to prepare an implant imitation were made and sent to the Tricomed company. The company began the process of creating the prosthesis.
First pictures of the prosthesis
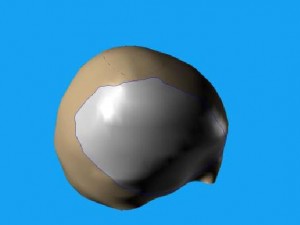
On 13/12/2012 I received the personalised prosthesis.
The doctor set the operation after Christmas, i.e. in late January and early February.
4. Course of the operation
2/14/2013 operation took place, I took part in it
The operation was carried out by two doctors:
1. G. Miliūnas – head of the neurosurgery department
2. V. Janušonis – the patient’s doctor
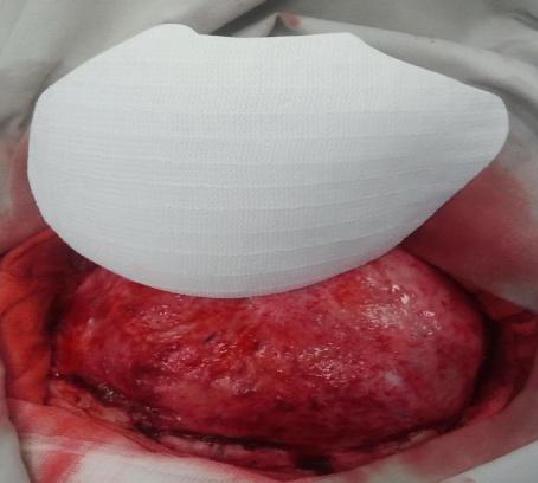
The operation lasted 3.5 hours. The implantation of the Codubix® CT prosthesis itself lasted about 30 minutes.
during the operation








5. Time after the surgery
1st day
The patient’s condition is stable, there is no visible signs of possible complications.
Computer image is taken – the implant is in place, no visible haemorrhage.
3rd day
The patient’s condition is stable. The patient is transferred to the general neurosurgery ward.
8th day
The patient feels well. According to the patient’s head does not hurt (without implants often had severe headaches) can sleep well (without implant could only sleep on one side and a special pillow) at any orientation of the head.
6. Doctor’s evaluation
The ward manager and the leading doctor are very satisfied with the results. The individually prepared prosthesis made a great impression on them – as a qualitative, precise and well-adjustable product. Such a large skull defect 10 x 14 cm could only be filled with Codubix® CT. The use of other products would not allow for the excision of an appropriate thickness and curvature of the implant, which could lead to many complications.
Violeta Senavaitienė
Matopat Representative – Lithuania
30/04/2013
1. Place – Kaunas (Lithuania)
Location of the operation:
Public facility, Lithuanian University Hospital of Health Sciences in Kaunas.
The clinic is the largest multi-profile hospital in Lithuania, and one of the most modern in the country.
The hospital employs more than a thousand doctors and more than two thousand medical personnel. The hospital can simultaneously accommodate up to two thousand patients. In fifteen buildings there are 34 profiled clinics, and 15 outpatient departments.

Date of the operation: 26/04/2013
2. Situation / circumstances
In January 2013 I conducted a presentation for neurosurgeons on Codubix® products. I presented all the possibilities and benefits they offer.
About two months later, I received a call from the hospital. They had a patient who needed the individual prosthesis.
The patient had a gunshot wound in the skull. The patient lost a large part of the skull (photos below). For about a month the doctors fought for his life. After a month it was necessary to restore the damaged bone. The product, which was available in the hospital – Tecres s.p.a Acrilic resin – was not suitable for such a serious damage. It was decided to prepare an individual prosthesis.
Once again I had to present all the possibilities of preparing the individual prosthesis.
3. Actions before the operation
On March 29, 2013 under my direction all the necessary computer images were taken and transferred to the Tricomed company. There began the production of the prosthesis.
Typical prosthesis Maximum size of the prosthesis Prosthesis needed for the given patient

3D model
Because the damage was very serious, the producer decided to make the prosthesis in two parts.
Dr. P. Kasprzak explains – the largest prosthesis met in the literature was 400 cm2. In our case – 280 cm2. It is the second largest case in the world (of course of the known cases).
April 25, 2013 I received the individually prepared prosthesis.
4. Course of the operation
The operation took place on April 26, 2013. I took part in it.
The operation was conducted by two doctors:
1. Associate Professor R. Vilcinis – head of the Craniocerebral Department
2. L. Kalasauskas MD – patient’s doctor
The operation lasted for about three hours. The adjustment of the prosthesis Codubix® CT took about 30 minutes. Parts of the prosthesis were connected by means of Aesculap titanium plates. Using the same Aesculap titanium plates the prosthesis was attached to the skull.
during the operation



preparing the place for the implant

after the implantation


before and after the operation


5. Time after the surgery
1st day
The patient’s condition is stable, there is no visible signs of possible complications. The patient is transferred to the general neurosurgery ward.
3rd day
The patient’s condition is stable, there is no signs of complications.
4th day
The patient’s condition is stable. The neurological condition improved – the patient began to respond to the environment, he began to move his legs and his fingers. From time to time there was a smile on his face.
6. Doctor’s evaluation
The Head of the Department and the patient’s doctor were very satisfied with the results. The prepared prosthesis made very good impression on them – it was of good quality, precise, easily adjustable. Such a large skull bone loss (a gunshot wound) could only be completed with an individually prepared prosthesis.
7. Problems / remarks
The hospital is very demanding as for the manufacturers and product representatives. Therefore, it took a lot of effort to get doctors to make a positive decision. This result was achieved only by working closely with the company employees and their operability.
(…) they affect up to half a million people in our country. If we add to this the number of family members caring for the people, that number will increase up to 1.5 million people directly related to the subject of chronic wound treatment (…)

The term “wounds” often evokes the notion of cut and stab wounds, which is a result of all sorts of crime fiction, novels and thrillers. These wounds of course require professional treatment and dressings but heal more quickly. It is much more difficult to treat so-called chronic wounds, which occur in up to half a million people in our country. If we add to this the number of family members caring for the people, that number will increase up to 1.5 million people directly related to the subject of chronic wound treatment, and thus – the principles of selection and dressing change.
Treatment of chronic wounds, or such as diabetic foot and pressure ulcers, and even burns, often lasts for months. It is very inconvenient for family members, as well as difficult for the person affected by this problem. This article is to encourage to become familiar with modern methods of chronic wound treatment in a moist environment, in accordance with principles developed by researchers. Let this article serve as an introduction to the topic and let it be some kind of hint, how in a modern way effectively and quickly treat chronic wounds.
Speaking of the modern chronic wound treatment, we do not recognise traditional dressings as bad. Traditional gauze dressings, bandages and plasters are good! No one questions their effectiveness, because they are perfect for the treatment of acute wounds (i.e. those resulting from mechanical reasons e.g. cuts, stab wounds, gunshot wounds and abrasions). In those cases sterile gauze dressings and plasters are most appropriate to be used.
EFFECTIVE CHRONIC WOUND TREATMENT
In case of chronic wounds (such as bedsores, burns, diabetic foot) as already as 40 years ago specialists discovered and clearly stated which conditions favour their rapid healing. This is the complete opposite to what traditional dressings provide. It turns out that a chronic wound will heal better if the following conditions are met:
- moist wound healing environment – promotes natural wound cleansing processes, regeneration of damaged tissues and reduces pain. This allows the wound to heal on average 50% faster;
- reduced pH value – lowering the pH value, the acidity of the wound environment increases, inhibiting bacterial growth;
- tightly closed wound (occlusion) – protects the wound from being infected by bacteria present in the patient’s environment. The use of special dressings of polyurethane foams also protects the wound against mechanical damage;
- stable temperature – stable temperature of about 37°C accelerates cell division, and thus regeneration of damaged tissues.
 FEATURES OF A PERFECT DRESSING
FEATURES OF A PERFECT DRESSING
Continuing research conducted by Georg Winter since 1962, William Tuner collected and summarised their results and presented them in 1979, defining the qualities of a perfect dressing. According to W. Turner a dressing, which, according to the modern (wet) wound healing model, will facilitate the healing process should:
- maintain optimum moisture in the wound,
- remove excess exudate and toxic components,
- isolate the wound thermally,
- allow gas exchange between the wound and the environment,
- be impermeable to bacteria and other microorganisms,
- be free from toxic particles and substances,
- provide protection for the newly formed tissues,
- be easily removed from the wound surface, without causing injury.
Dressings meeting the above criteria form a moist environment that favours important processes which take place in the wound, so that the healing process is about 50% faster with reduced sensation of pain and reduced risk of infection.
Why, despite the presence of a whole range of advanced dressings, the choice of the right one is so difficult?
Good identification of processes appearing during the wound healing process resulted in creating many specialised dressings with a number of very different characteristic features. Paradoxically, a large variety of dressings raises dilemmas about accurate selection in a specific situation. Remember that the decision to use a given dressing determines its effectiveness or lack thereof.
HOW TO CHOOSE THE DRESSING TO THE WOUND?
It seems that the choice of dressing must meet two basic criteria – we must remember that according to the modern wound healing approach there is no universal dressing that would meet requirements of every wound, and that choice must be aware, based on the correct diagnosis of the processes taking place in the wound and suitable for that characteristic features of the dressing.
To facilitate the correct dressing choice, you can use the wound classification based on the phenomena that take place in different phases of wound healing and based on that wound colour assessment.
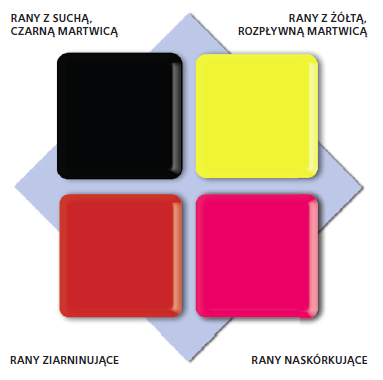
The scale consists of four colours respectively assigned to the specific stages of the wound healing process.
Selection of the dressing to the given wound while using the wound colour classification system becomes easier, because the wounds of the same type (colour) set similar challenges, and therefore require a similar procedure.
„BLACK” WOUND – NECROTIC TISSUE

OBJECTIVE OF THE TREATMENT:
- removal of necrotic tissue
WOUND CHARACTERISTICS:
- in form of dehydrated dead tissue
- necrotic tissue covers the entire wound or is present locally in form of patches
- exudate level – low (up to the point where necrosis turn into liquid discharge and separates from healthy tissue)
- necrotic tissue inhibits the healing process – it is the source of infection for healthy tissues, constitutes a barrier to the building new tissue
PROCEDURE:
- it is necessary to remove necrotic scab by a surgeon or in the autolysis process by the maintenance of a moist environment
RECOMMENDED DRESSINGS:
„YELLOW” WOUND – NECROLYSIS


OBJECTIVE OF THE TREATMENT:
- removal of necrotic tissue and preparing the wound bed for granulation
WOUND CHARACTERISTICS:
- cream colour of the wound – yellow, fibrous
- exudate level: high, medium, rarely low
PROCEDURE:
- maintain a moist wound environment
- control the level of exudate
RECOMMENDED DRESSINGS:
- Medisorb SILVER and SILVER PAD – infected wounds with high level of exudate
- Medisorb A – deep wounds with high or medium level of exudate
- Medisorb P – shallower wounds with medium level of exudate
- Medisorb P PLUS – shallower wounds with quite high level of exudate
- Medisorb H – moderate and low exuding wounds
- Medisorb G – infected wounds with low level of exudate (promotes wound cleansing by binding pre-hydrated dead tissue with microorganisms that colonise it)
„RED” WOUND – GRANULATING TISSUE


OBJECTIVE OF THE TREATMENT:
- maintain a moist wound environment conducive to granulation
- control the level of exudate
WOUND CHARACTERISTICS:
- wound in a bright red colour, moist
- uneven wound surface
- the tissue is delicate, sensitive to pain, susceptible to infection
RECOMMENDED DRESSINGS:
- Medisorb A, Medisorb P or Medisorb P PLUS – heavy and moderate exuding wounds
- Medisorb H – moderate and low exuding wounds
- Medisorb G – infected wounds with low level of exudate (promotes wound cleansing by binding pre-hydrated dead tissue with microorganisms that colonise it)
- Medisorb A – in case of infected wounds with high level of exudate
„PINK” WOUND – EPITHELISING TISSUE

OBJECTIVE OF THE TREATMENT:
- protection of new tissue
- stimulation of skin formation
WOUND CHARACTERISTICS:
- pink or white tissue appears on the wound surface
- epithelial cells migrate from the wound edges to the centre
PROCEDURE:
- encourage or support the process of skin formation
- maintain a moist wound environment
- protect against mechanical damage
RECOMMENDED DRESSINGS:
- Medisorb H – moderate exuding wounds
- Medisorb F – low exuding wounds
Hanna Szymkiewicz
European Centre for Long-Term Care
A wound is a skin break, which may extend to deeper tissues and organs. The cause of the wound can be internal and external factors associated with physiological disturbances. The breadth and depth of the wound depends on the causative agent, its strength and areas it affected.

Division of wounds due to the causative agent:
>> exogenous factors:
- mechanical (cut, stab, mashed, gunshot wounds)
- thermal (burns, frostbites)
- chemical (chemical burns)
- electrical (burns)
>> endogenous factors
- ulcers (leg ulcers, pressure sores, diabetic foot) – e.g. impaired circulation
Division of wounds due to the healing time:
- sharp – less than 8 weeks
- chronic – more than 8 weeks
Division of wounds due to the way healing:
- acute wounds – cuts, surgical wounds with even edges and in which there is no substantial loss of tissue. Such wounds are closed with sutures, staples or a dressing, and the wound is healed by first intention and lasts about 6-7 days. It is the most preferred way of healing, and is referred to as primary healing.
- chronic wound – wounds where there is a significant loss of tissue and / or infection. In this case, it is not possible to bring the wound edges together. This type of wound healing by granulation (secondary intention) – the inflammatory phase is followed by proliferative phase, in which the tissue loss is filled with granulation tissue. This process is called secondary healing.
Secondary healing
Secondary wound healing concerns chronic wounds – including bedsores, ulcers, and complicated wounds caused by exogenous factors, such as complex surgical wounds. There are three phases in this healing:
- inflammatory phase (purification)
- proliferation (granulation)
- maturation
The inflammatory phase is characterised by an inflammatory reaction and pain. The body is trying to destroy the bacteria that get into the wound after the discontinuation of the skin. Exudate appears. The dead tissues are excreted out or absorbed by the organism. The wound gets covered with blood clot, which protects it from germs.
In the proliferation phase the exudate is reduced, vessels get narrower, and this is followed by granulation – filling the tissue loss and epithelialisation – the wound is covered with new epidermis.
In the maturation phase the rebuilding process of the newly healed wound takes place to get the strength similar to the intact skin.
The process of healing and its duration depends on many different factors: the general condition of the patient: the age, nutritional status and co-existing diseases; the type of the injury, its location, its closure way, its cleanliness and the time that has passes since the injury to its dressing.
Jolanta Machańska
Educator in Diabetes
Diabetes is a major and increasing health problem. It affects people at any age and in all countries. It is a disease that lasts from its inception throughout the patient’s life, usually for a few dozen years.
It is one of the main direct and indirect perpetrators of disability – blindness, kidney failure, gangrene and amputation of the lower limbs, the severity of coronary heart disease and stroke and early human mortality.

Complications of diabetes can be acute i.e. states where deep metabolic disorders appears suddenly, usually combined with disorders of fluid-electrolyte balance and acid-alkaline balance, fast leading to a significant impairment of general condition, loss of consciousness and sometimes death.
The second group of complications are chronic diseases i.e. specific groups of disorders and symptoms of being a clinical exponent of changes in vessels, nerves and other organs that appear along diabetes and contribute to disability and premature mortality.
ACUTE COMPLICATIONS
Acute metabolic disorders – diabetic comas, in fact, is not a complication of diabetes, but the consequence of insulin deficiency. In the period before the discovery of insulin they were regarded as the final stage of the disease. Currently they appear only if there is no or improper treatment. Diabetic coma can have a different course, which results from separate pathogenic mechanisms leading to this condition.
At this time, the following types are distinguished:
- diabetic ketoacidosis
- severe diabetic hypoglycaemia
- hyperosmolar nonketotic coma
Diabetic ketoacidosis
Occurs most often (mainly in patients with type 1 diabetes – juvenile diabetes, absolute insulin deficiency) and the best known. It develops in the course of diabetic ketoacidosis, which affects mainly people completely devoid of pancreatic islet beta cells.
Causes:
- infections, especially purulent ones where rapidly increasing insulin resistance results in increased demand for insulin
- severe systemic diseases such as myocardial infarction, stroke, pneumonia, and major surgeries
- pregnancy with insulin resistance and increased insulin demand
- lack of patient education – often ignorant patients discontinue insulin delivery due to the loss of appetite (fever) and fear of hypoglycaemia
The clinical picture is quite diverse, and the intensity and type of common ailments and symptoms are not always formed parallel to the results of laboratory tests.
Symptoms may be presented in several groups:
Consequences of dehydration: very large thirst, polyuria reaching a few litres a day, dry tongue and mucous membranes, dry skin, soft eyeballs. Initially there is an increase in body temperature, which, if there is no infection, later turns into hypothermia, a drop in blood pressure, especially in elderly people, in extreme cases, loss of pulse and bruising of the distal parts of the body.
Gastrointestinal disorders: dreg type vomiting, abdominal pain – in extreme cases, false peritoneal symptoms (ketotic abdomen), enlargement of the liver.
Respiratory disorders: Kussmaul breath (breath of a chased dog) – deep and laboured characterised by four phases: inhale – pause – exhale – pause, acetone odour can be felt in the breath – the smell of rotten apples.
Consciousness disorders: four stages can de distinguished in the developing ketoacidosis:
- tiredness, impaired balance and vision
- state of somnolence, abnormal thinking
- deep sleep with preserved reactions to painful stimuli: the weakening of physiological reflexes
- deep neurological coma with the reduction of response to painful stimuli and physiological reflexes
Treatment
Once the diabetic coma or being at risk of it is diagnosed, the patient should be immediately sent to the nearest hospital. It would be perfect if there was diabetes ward with intensive care room in the hospital.
The treatment of diabetic ketoacidosis includes:
- insulin delivery – preferably by continuous infusion by means of a pump
- supplementing fluid and electrolyte insufficiency
- use of alkalising medicines
- treatment of complications
Hypoglycaemia
Another condition which is a complication not of diabetes itself, but the treatment. Blood hypoglycaemia of various severity are the most common complications arising in people treated with insulin; therefore, anyone who comes into contact with diabetics, should have knowledge about hypoglycaemia.

Causes:
- errors in insulin therapy: determining too much insulin, a mistake in the measurement of the dose of insulin, too late reduction of the dosage, when patient’s body weight decreased, diet therapy proved to be more accurate, infection was removed
- the pursuit of too rapid metabolic levelling out by a large increase in the dose of rapid-acting insulin, or despite the absence of conditions for this
- errors in nutrition: too long intervals between meals, too little carbohydrate in the meal, alcohol
- disorders of the gastrointestinal tract: vomiting, diarrhoea, abnormal gastric emptying
- changes in the absorption of insulin: change of injection place, the muscles in the thigh, where insulin is administered (march immediately after the administration of insulin), heating the injection site (shower after the injection), change in the depth of the puncture, accidental intramuscular or intravenous injection
- starting a new vial of insulin: the insulin may be more active than previously used, stored at room temperature
- reduced need for insulin due to emotional hyperactivity, menstruation, hormonal disorders
- intake of glucose lowering medicines: acetylsalicylic acid, beta-blockers
- increased physical activity
- natural remission of diabetes
Signs and symptoms:
There are many symptoms of hypoglycaemia. Particularly rich and varied individually is the subjective symptomatology. Symptoms are more limited objective and non-specific. Time and rate of increase of symptoms depend to a large extent on the type of insulin, the amount of injected dose and the daily dosage schedule.
In blood hypoglycaemia we can distinguish:
Neurovegetative symptoms (catecholamine): agitation, fatigue, skin pallor, sweating, dilated pupils, tachycardia, a moderate increase in pressure. Symptoms present at glucose concentration of 65 – 55 mg/dl.
Neuroglycopenia symptoms are caused by a reduction of transmission of glucose to the brain. They can be divided into mental symptoms: anxiety, abnormal thinking, cognitive disorders, inability to concentrate, personality changes, amnesia, manic behaviour, delirium, and neurological symptoms: slurred speech, vision, clonic and tonic spasms, overactive tendon reflexes, positive Babinski sign, loss of consciousness. These symptoms occur when the glucose concentration reached approximately 45 mg/dl.
The neurovegetative symptoms are a warning to the patient of threatening neuroglycopenia and are indication for acute prophylactic – eating a meal or sugar. Within time these symptoms of diabetes are reduced or even disappear.
Treatment

The treatment deals with immediate administration of carbohydrate in an amount increasing blood glucose. Mild hypoglycaemic states are treated by the consumption of additional food, if necessary, a few lumps of sugar that a diabetic patient should always have on him/her.
In states of unconsciousness 1 mg of glucagon should be injected. Upon regaining the consciousness, the patient should be fed and watered with sweet liquid until return to normal glucose level. If we are able to give drugs intravenously, the patient should get 1 mg of glucagon subcutaneously, then we give 5 or 10% glucose until the glycaemic stabilises. In case of insulin overdose, after transient improvement the hypoglycaemia may occur again. Such a patient requires hospitalisation. In most cases of hypoglycaemia the prognosis is good. It can be quickly and easily controlled. However, repeated hypoglycaemic states can cause chronic threat due to the extinction of warning signs and abnormal neurohormonal regulation of glycaemic homeostasis.
Very severe hypoglycaemic shock can lead to death or cause permanent damage to the central nervous system and permanent maintenance of mental and neurological symptoms. In diabetic patients treated with insulin, the appearance of hypoglycaemia state is an alarming condition and requires prompt clarification of the cause of this complication, and if necessary correction of the treatment. Appropriate therapeutic programs should implement, taking into account the patient’s involvement in order to minimise the risk of this complications.
CHRONIC COMPLICATIONS OF DIABETES
The characteristic feature of organ changes, referred to as chronic complications of diabetes, is their slow and long-term development. Therefore, they disclose as well-defined clinical syndromes or less specific symptoms of the disease at a later stage, and only then they can cause disability and life threat. For these reasons they are called late complications of diabetes. Long-term asymptomatic evolution of the changes bears the danger of underestimating the negative impact on the prognosis of diabetes.
The major chronic complications of diabetes include:
- changes in the vessels – angiopathia diabetica, changes affect both large vessels – macroangiopathy, and small vessels and capillaries – microangiopathy
- changes in peripheral nerves – neuropathy
- changes outside the circulatory and nervous system: gastrointestinal tract, skin, motor organ, lens
Microangiopathy
Small vessel disease are diabetes-specific changes in the capillaries, which are present in all organs, in which the vessels have a basal membrane e.g. changes to the capillaries in the eyes and kidneys cause such significant damage to these organs that it is disclosed in the form of characteristic clinical syndromes. These syndromes are the cause of disability, and even premature death.
Treatment
The treatment should be initiated by the correction and providing the best possible clinical and biochemical indicators. It is important to introduce the change relatively slowly. Too violent attempts to stabilise the diabetes may lead to accelerate the progress of changes. In the symptomatic treatment vessel sealing preparations are used.
Prevention refers to optimal diabetes treatment from the beginning of the disease with the use of contemporary therapies. It is recommended to take early prevention in form of regular evaluation of the ocular fundus and kidney function.
Macroangiopathy
Large vessel disease whose anatomical substrate is atherosclerosis, and to a lower extent – hardening of arterioles. Changes in the arteries and arterioles are very common in diabetes and appear earlier and are more intensive, which in turn causes premature death or disability. They are especially common among patients with type 2 diabetes, especially in the elderly.
Characteristic features of the large vessel disease in people with diabetes:
Coronary heart disease is most common and is the leading cause of death in diabetic patients. A characteristic feature is asymptomatic and painless myocardial infarction. Approximately in 8% of people with diabetes, both women and men, an ECG test shows abnormalities that might be the evidence of past cardiac necrosis. This applies mainly to patients with long-lasting diabetes, in whom coronary artery disease coexists with other late complications of diabetes, especially diabetic nephropathy.
Cerebrovascular disease is a collection of non-specific for diabetes neurological syndromes, which are the clinical expression of brain ischemia as a result of atherosclerosis and hardening of the arterioles. Cerebral haemorrhages rarely occur in diabetic patients. Thromboembolic changes prevail, which can cause cerebral infarction and softening. Approximately in half of the diabetic patients after stroke also microangiopathic, retinopathic and nephropathic changes appear.
Leg artery disease is the equivalent of arterial occlusive atherosclerosis. The name “leg artery disease” was introduced the WHO Expert Committee on Diabetes to note that:
- vessel changes in diabetic patients are more varied and apart from the atherosclerosis of large vessels include also the sclerosis of arterioles and small vessel disease, and therefore are more extensive and reach the end of the limb
- in diabetes the changes in a specific way focus in the lower limbs; the changes are here more advanced than in other sections of the vascular system.
Occlusion of bigger arteries or arterioles by a sudden or more slowly forming clot causes the necrosis of the most remote sections of the foot or foot gangrene – gangrene pedis diabetica that due to the complexity of its pathogenesis, should be treated as a separate clinical syndrome. Leg artery disease can result in severe disability.
Diabetic neuropathy
Various kinds of damage to the peripheral nervous system, and its clinical forms are:
Symmetrical sensorimotor peripheral neuropathy characterised by the earlier damage of sensory nerve, lower – of the motor nerves; the lower limbs are predisposed to these changes, and rarely the upper limbs.

The clinical picture
In the initial period: tingling, burning, less impetuous and burning pain in the feet. The symptoms are at rest, intensifying at night under the influence of heat. Sometimes there may appear thermal paraesthesia and the sensation of cold, despite the fact that the feet are warm. Often the “restless legs” symptom appears, forcing them to constant move and change of position.
Mild neuropathy, in which symptoms intensify. Particularly troublesome is the sensation of burning feet. At the same time there are areas with reduced surface sensation, localised mainly in distal sections of the limbs, resembling due to its scope “gloves” or “socks”.
Severe neuropathy causing all forms of disorders to superficial sensation and vibrations. The sensory disturbance is accompanied by physiological reflexes. There appear areas of pain hypoaesthesia, favouring painless injuries. Later on, paresis and muscular atrophy appear, usually affecting foot extensors, small foot muscles, while in the upper limb they affect muscles innervated by the ulnar nerve. The changes in the muscle are accompanied by neurotrophic changes in osteoarthritis.
Focal neuropathy (mononeuropathy) – this complication involves damage to a single sensory or motor nerve, or to several nerves simultaneously, but then these changes are not symmetric and affect nerves in different areas of the body. It is assumed that its immediate cause is sudden ischemia resulting from closure of a nutrient vessel. The main symptoms of mononeuropathy are very strong radiating pain characteristic of the busy nerve and paresis. Mostly the changes affect: the femoral, sciatic, peroneal, median and ulnar nerve. Despite dramatic progress complete recovery can be seen within a few weeks or months.
Autonomic neuropathy is a group of symptoms affecting the autonomic neurons of either or both of the parasympathetic and sympathetic nervous systems.
The clinical picture consists of various syndromes reflecting dysfunctions of individual organs and systems.
Diabetic foot syndrome is a collective term for changes that occur on feet in patients with long-standing diabetes. Their main reason is diabetic specific damage to foot nerves – diabetic neuropathy. It is accompanied by changes in the joints, ligaments and foot bones as well as vascular changes, with causes that the foot is shortened, widened, the longitudinal arch gets deeper. Pressure places appear on the sole, and the reaction of the skin to them is the creation of calluses and cracks in the skin, which are the starting point for infection and foot ulcers.
Pathological changes and clinical symptoms on the lower limbs and feet:
- Changes in the vasculature: atherosclerosis, hardening of the arterioles, microangiopathy of foot tissues, ischemia of soft tissues and bones, formation of infected or not infected necrosis.
- Changes in the innervation of the foot: the loss or impairment of sensory innervation (decrease or loss of pain sensation of pain, temperature, touch, vibration), motor activity (impairment of muscle tension and foot movements, muscle atrophy), autonomic activity (impaired regulation of blood flow through the foot); trophic disorders in the joints (formation of deformations, impaired sweating).
- Skin changes: pale or grey-blue skin, papery, dry, cracked, non-elastic, hair loss, abnormal growth of nails, calluses, necrosis and ulceration.
- Changes in the muscle: muscle weakness, changes in tension, muscle atrophy, contracture.
- Bone abnormalities: bone loss, necrosis, deformations.
Treatment depends on the degree of foot damage. The diagnosis of diabetes begins with conservative treatment. The aim is to metabolic equalisation of the disease, avoid, and preferably completely give up smoking and alcohol consumption, implement an intensive program of general physical exercise and especially foot exercise and their care.
Elżbieta Szwałkiewicz
National Consultant in Nursing Chronically Ill and Disabled People
One of the indicators used to assess the quality of long-term care of an immobilised person is the skin condition in areas exposed to constant pressure. It would seem that nurses know everything on the prevention of pressure ulcers, and that is why I wonder what is the reason for such a high incidence of pressure ulcers in people who are under constant nursing supervision.

The scale of the problem entitles me to claim that in our country we have common and very serious failings in the care of the sick and disabled, both in stationary health-care and social assistance, as well as in home conditions. These neglects are the cause of immense suffering and generate substantial costs of treatment and care.
There have been many publications on the subject of pressure ulcers referring to numerous medical research and statistics. They repeat the same key information:
- the major etiological factor is the pressure on tissue located over bone prominences, leading to the development of necrosis and then to ulceration,
- skin damage occurs as a result of repeated pressure exceeds the average pressure in skin capillaries (32 mmHg), the impairment of sensation is a contributing factor,
- the formation of pressure ulcers is accelerated by skin maceration, which is a consequence of increased humidity due to urine and faecal incontinence or perspiration,
- the most common location is around the sacrum, ischiadic tubers, trochaners, ankles and heels,
- each immobilised patient is at risk of pressure ulcer formation,
- modern technologies ought to be used to reduce the pressure on the skin, such as specially designed mattresses, pillows, textiles and equipment for sliding movement, modern protective and therapeutic dressings, and aids absorbing urine,
- the treatment cannot be focused on the topical management of decubitus ulcer.
Basic principles relating to prevention:
- proper nutrition – adequate intake of protein, calories and fluids will prevent the occurrence of negative nitrogen balance, weakness and dehydration,
- reduction or elimination of pressure and friction on the skin – this effect is achieved through the use of pressure relief mattresses and pillows, frequent change of body position, application of proper rules for lifting and moving patients,
- strictly comply with the basic care principles of people with incontinence (also the faecal type), including:
- daily washing and cleaning after every contamination with excretions,
- systematic control of skin condition in areas exposed to moisture,
- using absorbent products adequate to the level of micturition,
- preventing skin inflammation through the use of special protective dressings,
- protecting the skin against overdrying and irritants (urine and sweat) through the use of appropriate skin care products.
Modern approach to the treatment of pressure ulcers and other chronic wounds favours wound healing in a humid environment with the use of various specialist dressings, which are applied depending on the type and the location of the wound.
Scientific studies and practical experience have shown that increased moisture in the wound stimulates epidermisation, and this, in turn, stimulates the growth of connective tissue underlying the skin. Specialist dressings compared to conventional gauze dressings also affect the rate of healing. They prevent the damage to the young epidermis during each dressing change, and they contain substances that affect the treatment and healing of wounds. Not to be underestimated is the fact that effective protection of the interior of the wound against external factors, and to perform normal hygiene procedures without changing the dressing.
Therapeutic proceedings (including the selection of a dressing) and the cost depends on the type of wound and the stage of healing . Some wounds are treated for many months, sometimes over a year. There are often problems in the healing process, and the most dangerous of them cause infections. An unsecured wound may be infected with bacteria, viruses or fungi. They proliferate spontaneously and poison tissues with their secretions. The wound infection can spread quickly up to the form of sepsis, which threatens the patient’s life. The cost of treating infected chronic wounds significantly increases mainly due to the need to use more specialist dressings and the use of expensive antibiotics.
As a national consultant I observe with great concern that the number of people who suffer from pressure ulcers and other chronic wounds is not decreasing despite years of educational campaigns. The responsibility for this situation falls not only on the nurses but also on those responsible for creating the conditions for the care of sick and dependent people, and the National Health Fund as a payer financing the costs of treatment. It is difficult to understand the fact that the National Health Fund does not require health care centres to report on patients with bedsores and the course of treatment. Isolating procedures concerning the treatment of bedsores, and leaving the treatment costs within the institution in which they occur, would highly affect and activate the creation of suitable conditions for the prevention of pressure ulcers. It should of course take into account the fact that some chronic wounds are not the result of negligence but result from the patient’s physical condition; most often it relates to end-phase of long-term biologically devastating neoplastic disease.
As part of my own professional practice I was able to watch quite remarkable effectiveness of modern specialised dressings in the treating of pressure ulcers. Of course, the nurses should be aware of all the known methods of chronic wounds treatment, not only of pressure ulcers but also ulcers, malignant ulcers, diabetic foot ulcers and burns. The bottom line is to be aware that it is unacceptable not to obey the basic prevention principles and to expose the patient to the formation of pressure ulcers or other chronic wounds. Both health and financial consequences of economising on absorbent products and protective dressings are very serious, not only for the patient but also for the nurses and the unit they work for.
Renata Kobierska
Director of the Nursing Home in Kalisz
Types of diabetes
Diabetes is a result of lack of insulin (a hormone produced by the pancreas) in the body. The role of insulin is comparable to the role of the key – thanks to it we get into the apartment, and thanks to insulin sugar (glucose) can get into the body’s cells where it is converted among other things into energy. If there is lack of insulin in the body, sugar builds up in the bloodstream.
Currently, there are two prevalent types of diabetes: type 1 and type 2. The causes of this condition are different depending on the type of the disease.

Type 1 diabetes, formerly insulin dependent diabetes or juvenile diabetes, is caused by a complete lack of insulin due to the damage of appropriate cells of the pancreas. It occurs mainly in children and adolescents, hence its name. The emergence of the disease is not fully known. We only know that it is genetically determined, resulting in impaired immune mechanism and further in damage to the beta cells of the pancreas.
Type 2 diabetes, formerly noninsulin-dependent diabetes, is the most common form of the disease. The cause is usually impaired insulin secretion by pancreatic beta cells or the use of insulin by tissues. This diabetes occurs most often in the elderly people, obese, or with other metabolic disorders. In the early stage of the disease insulin is secreted in increased amounts, but at the same time the amount is insufficient for the increased needs of the body (insulin resistance).
In the literature there are many definitions of diabetes, and one of them says that it is a group of various genetically determined and acquired metabolic disorders that are characterised by glucose intolerance and hyperglycaemia, and over time the emergence in the vascular system, nervous system and other organs of changes referred to as chronic complications of diabetes. The cause of impaired glucose tolerance is the lack of insulin or its inappropriate tissue action. The name “diabetes” according to the new classification means a disease with a complete clinical picture, and mild carbohydrate metabolism disorders are called impaired glucose tolerance. 1
However, according to J. Tatoń diabetes is “a large group of diseases and metabolic disorders of various etiology, characterised by a constant, pathological fasting hyperglycaemia, between meals or just after a meal, resulting from the failure of insulin secretion by pancreatic beta cells or impaired response of cells, tissues and peripheral organs”. 2
In 1997 the American Diabetes Association developed a new division of diabetes, which was modified in 2003 and is now it looks as follows:
- type 1 diabetes – the destruction of beta cells leading to absolute insulin deficiency
- type 2 diabetes – a progressive disorder of insulin secretion and insulin resistance
- other specific types of diabetes – caused by genetic defects of beta cell function and insulin action, by exocrine pancreatic diseases, certain drugs or chemicals
- gestational diabetes – diagnosed during pregnancy
Classification of type 2 diabetes by Tatoń:
1. Genetic conditioning:
- occurring within a family
- with the occurrence of erythema after chlorpropamide and alcohol
- associated with syndromes caused by genetic disorders
- type 2 diabetes syndrome in young people
2. Nutrition conditioning:
- hyperplastic obesity
- hypertrophic obesity
- without obesity
3. Determinants of disturbed cell reactivity to insulin:
- with an excess of hormonal “anti-insulin” factors
- with impaired insulin receptor function
Each of these subtypes can be divided into type 2 diabetes treated with:
- diet alone
- oral hypoglycaemic medicines
- insulin 3
Symptoms
Type 2 diabetes has often latent asymptomatic course, so it cannot give characteristic symptoms. This disease is like a “mask” and as a result it is often diagnosed only when symptoms get worse or when another illness appears. The “mask” symptoms characteristic for type 2 diabetes include:
- skin symptoms – itchy skin, especially in the genital area, boils, thrush, fungal nail infections, poor wound healing, xanthomas, hair loss
- gynaecological symptoms – vaginal bacterial infection, vaginal thrush, menstrual disorders, impotence
- nervous system symptoms – numbness, stinging, burning, loss of sensation – especially in fingers and toes, nocturnal leg cramps, weakness of one of the nerves
- fatigue, weakness
- blurred vision
- miscarriages

The typical symptoms of type 2 diabetes include:
- general weakness
- increased thirst
- increased appetite
- thinning
- polyuria
- infections
- skin inflammation and itching 4
Every cell in our body need glucose i.e. sugar, which is the source of energy and affects the normal functioning of the brain, muscles, liver, kidney and heart. The glucose to penetrate into the cells requires insulin. When cells become resistant to the hormone, the sugar cannot get into them, but circulates in the bloodstream. This causes an excessive amount of glucose in the blood (hyperglycaemia) and so-called cell hunger. The body in defending itself from the lack of sugar triggers the mechanisms of increased appetite, but due to the lack of insulin the glucose from food cannot get into the tissues – is excreted in the urine. Undiagnosed type 2 diabetes leads to severe complications. Can cause atherosclerosis, heart attack or stroke i.e. conditions associated with the damage to large blood vessels. The second type of complications results from the damage to small blood vessels. These include, inter alia, retinopathy (eye disease), which can lead to blindness. Patients may also suffer from kidney failure and circulatory disorders and innervation of the lower limbs. They lead to the development of so-called diabetic foot ulcers – wounds and ulcers occurring on the leg. If this condition is not healed in time it may lead to amputation.
How to live with diabetes
It is possible to live a normal life with diabetes provided that a few basic rules are obeyed:
- education i.e. consciousness – in diabetes, as in any other disease, the patients are responsible for their own health
- nutrition – drug therapy with appropriate diet does not differ from the one recommended for healthy people
- physical exercise – walking, playing sports should become a habit, because it provides good physical form of every human being
- medicines – modern treatment consists of therapy that allows to restore similar processes that take place in the body of a healthy man
Literature:
1. A. Czyżyk, Encyklopedia chorego na cukrzycę, PWN, Warszawa 1992.
2. J. Tatoń, Poradnik dla osób z cukrzycą typu 2, PZWL, Warszawa 2002.
3. J. Tatoń, Diabetologia kliniczna, PZWL , Warszawa 1986.
4. P. Hien, Cukrzyca, krótki kurs diabetologii, Sprinter, PWN, Warszawa, 1997.
Causes
The diabetic foot syndrome deals with changes appearing on the lower extremities in patients with diabetes.
The cause of the diabetic foot syndrome are changes in the blood vessels (ischemia), and damage to the nerves (neuropathy). Deterioration of vascularisation and innervation in diabetic patients usually progress simultaneously, but only one of these changes is dominant. The dominant factor determines the type of the diabetic foot syndrome, and so can be distinguished: ischemic diabetic foot syndrome or neuropathic diabetic foot syndrome.
Figure: diabetic foot syndrome – classification as for the dominant factor
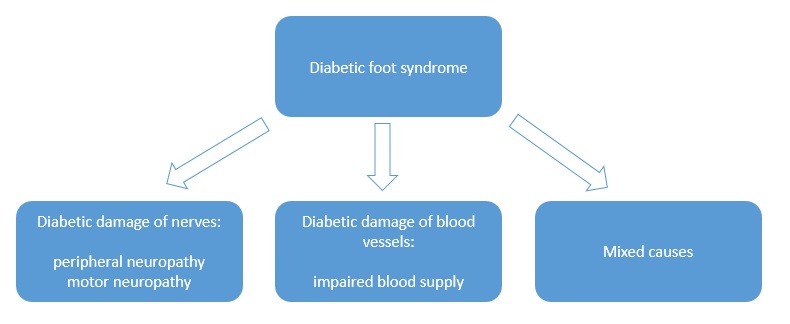
Peripheral neuropathy i.e. peripheral neuritis – is one of the complications of prolonged hyperglycemia and affects both somatic and autonomic nerve cell projections in both legs. The patient has reduced sensation of pain, temperature and touch in the affected leg, and since feels no pain after an injury or compression, the skin is often damaged and ulcers are formed, which are often not noticed early enough and thus start to be treated too late. Late detection of the ulcers may be then too advanced to be successfully treated.
Motor neuropathy causes loss of muscle and foot tendons and, consequently, destruction of the joints. This in turn leads to the concentration of workload on a few small areas of the plantar surface, and further to the formation of callus. The final step of these changes is foot deformation.
Angiopathy i.e. damage to blood vessels – blood supply disorders are characterised by abnormal blood flow in the legs especially tibial and fibular artery. Uncontrolled diabetes favours the development of arterial diseases. The control of blood glucose content is one of the prevention ways, it is also a precondition for starting the process of wound healing.
Therefore, we can distinguish:
- neuropathic foot ulcers, which constitute two thirds of all diabetic foot ulcers
- angiopathic foot ulcers (~ 10%)
- mixed foot ulcers (~ 25%)
Risk groups
- People with diabetes mellitus.
- People with undiagnosed diabetes!
This disease affects mostly people with type II diabetes i.e. the one not requiring insulin injections.
The complication in for of diabetic foot is present in approximately 20% of hospitalised patients because of diabetes, and is the cause of 50% of all limb amputations performed in surgical wards.
Symptoms
Neuropathic diabetic foot
The predominant symptoms:
- loss of sensation to touch, pain and temperature
The patient does not feel the presence of a malicious stimulus such as a cut, burn, hurting by wearing tight shoes, the presence of a foreign body in the shoe. Insensitivity to pain is the basic element causing the formation of ulcers on the foot sole. The neuropathic diabetic foot is warm, with preserved flow in the arteries, but the foot joints and bones are deformed.
In some patients the changes appear in the joints and are formed by gradual destruction of small joints of the foot which results in considerable distortion of the feet. It is necessary then to wear special shoes made upon an individual order. Wearing normal ill-fitting shoes very often leads to the formation of ulcers.
Ischemic diabetic foot syndrome – angiopathic
The predominant symptoms:
- increased sensitivity to pain
The main symptoms are: pain intensifying usually at night, often accompanying painful muscle cramps, tingling or numbness in the leg.
Depending on the level of stenosis and occlusion of arteries in the lower limb, necrosis appears on different areas of the foot.
The most severe form of the disease is the closure of large arteries in the lower limb above the knee. This results in tissue necrosis in the foot, and sometimes also in the lower leg. Necrosis affects mostly toes. Ischemic diabetic foot is characterised by preserved innervation while simultaneous impaired blood supply in the limb.
An untreated diabetic foot syndrome leads to the amputation of the limb.
Location
In patients with diabetic neuropathy ulcers are located primarily in areas of repeated injuries and affect usually the plantar surface of the foot around the metatarsal bone, heel and toes. Usually the neuropathic ulcers are painless.

In addition, as a result of neuroarthropathic disturbances, the foot is distorted in a characteristic way – grooved feet, mallet toes, changed way of walking, and in over-loaded points in the calluses (corns) are formed that can later cause non-healing wounds and ulcers.
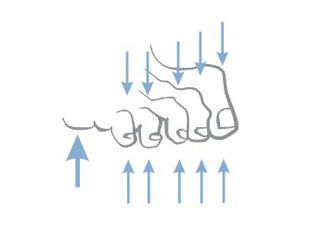
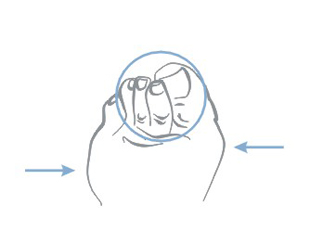
In the case of ischemic diabetic foot chronic hypoxia causes that the foot begins to die – it swells, ulcers, necrosis and cracks appear, nails get deformed and soft tissues disappear and the whole foot becomes blue.
Treatment
A specialist in the field of diabetes, surgery (including vascular surgery) and orthopaedics is the competent person for ordering treatment. Nurses also actively participate in the therapy. The most important thing is to keep sugar level in blood in optimal physiological limits.
The treatment is both causal and local.
Wounds are surgically debrided, narrowed blood vessels are unblocked, various vascular grafts are used to allow bypass clogged arteries which improves blood flow in the foot. Along with the surgery blood sugar in the body is controlled and medicaments facilitating the treatment are dosed. In addition to insulin and antibiotics the patient receives medicines that improve blood circulation in the limbs, reduce blood viscosity, enabling to reach the ischemic structures, improve wound healing and scarring. Also appropriate diet is recommended.
Prevention
It most essential in the prevention of diabetic foot development is the proper treatment of diabetes, the control and maintenance of a normal blood sugar level.
After diagnosing diabetes the patient should:
- quit smoking
- gently and carefully take care of the feet
- systematically control the circulation and innervation of the feet
If there are foot lesions, early physician intervention often prevents the need of amputation of the lower limb.
Everyday foot care in people with diabetes should consist of:
- everyday observation – controlling blood flow and sensation, washing in warm (not hot) water, gentle and careful drying – especially the space between toes
- care for nails – regular trimming (but not too short)
- careful selection of shoes – should be sufficiently wide, the right size (patients with neuropathy, due to the worsening of sensation tend to buy too small shoes, smaller than the ones worn so far), the heel should be low and wide, shoes with laces are recommended
- before putting on shoes the patient should check whether inside there are no sharp objects, outstanding seams or rolled inserts
- wear non-binding and non-elasticated socks made of natural fibres (too tight socks can impede blood circulation)
- protect the foot against excessive: soaking , exercises or heating (for example by means of an electric blanket or other energy sources)
- do not use ointments on foot corns – unless your doctor tells otherwise
Any observed changes in the foot, such as swelling, colour change, loss of sensation should be consulted as soon as possible with a doctor.
Even minor cuts, skin cracks and wounds cannot be ignored and always need to be secured with sterile dressings and shown to the doctor during control visits. If there is no progress in the healing it is recommended to urgently consult the doctor.
>
Causes
The causes of leg ulcers are diverse, internally complex and almost exclusively of endogenous-internal origin.
Without a doubt, however, the most common cause of leg ulcers is venous hypertension and arterial insufficiency.
Other possible causes of leg ulcers:
- hypertension: necrotising vascular dermatitis – necrotic angiodermatitis (Martorell syndrome)
- infections: osteomyelitis, tuberculosis, pyoderma gangrenosum, leprosy, insect bites
- vasculitis: polyarteritis nodosa, rheumatoid arthritis
- haematological disorders: haemolytic anemia, fibrinolytic disorders
- neurological disorders: poliomyelitis, peripheral neuropathy (diabetes)
- cancer: mixed basisquamous carcinoma (Marjolin’s ulcer), melanoma, Kaposi’s sarcoma, lymphoma
Ooccurrence
- 75% of all vascular ulcers are the result of venous hypertension – venous ulcers
- 15% is generated as a result of atherosclerosis – mixed ulcers
- 10% is arterial ulcers
Venous ulcers are caused by severely impaired activity of leg veins. In advanced venous insufficiency of the lower limbs, venous circulation in the lower limbs is disturbed and venous valves are damaged – which results in congestion and increased pressure in the veins. Valves control the blood flow so that it flows only in the direction towards the heart, not to move back. In case of damage or malfunction of valves blood flows back to the lower limb. Blood pressure in the venous system increases, which, if untreated, causes further damage to the valves and superficial veins. Walls of veins lose their flexibility and elasticity, get thicker. For the purpose of treatment and prevention of recurrence of ulcers, it is very important to identify the locations of venous insufficiency.
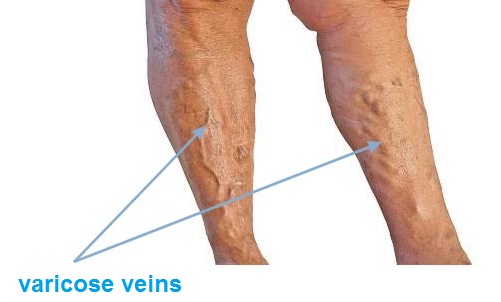
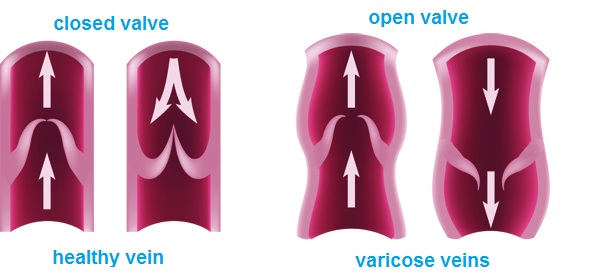
Risk group
- obesity
- work in a seated or standing position, leading to the stagnation of blood in leg
- hereditary factors – presence of varicose veins in parents
- age, mostly at risk are people over 60 years of age
- sex, statistically varicose veins are more common in women than in men
- number of pregnancies (the more births the greater the risk of varicose veins)
- constipation
- flat feet
- oral contraception
- tallness
Symptoms
The initial phase of venous insufficiency: feeling of heavy legs, especially in the evening, the emergence of the so-called spider veins and reticular veins. The next stage in the development of the disease are: emerging swelling around the ankles, then also swelling of the entire lower leg. Initially the swelling disappears after a night rest, and then becomes constant. After some times varicose veins may occur i.e. permanent extension of superficial veins.
In advanced venous insufficiency of the lower limbs trophic skin changes appear as well as discoloration, spots and hardening. Then itching appears, bumps, cracks, skin covering varicose veins is damaged, which inevitably leads to the formation of difficult to heal wounds known as leg ulcers.
Location
- Typical venous ulcers are located above the medial malleolus leg.
- Ischemic ulcers (arterial) are often found on the back of the toes, on the heel, or on the front surface of the shin.
- Rheumatic ulcers usually involve the side and back surface of the rest of the lower leg and the ankle area.
Where to seek help and advice
Of course, in the first instance go to your GP who should refer you to a specialist surgeon. Currently, the best method of diagnosing venous insufficiency is to perform an Colour Doppler ultrasound test.
Treatment
In case of ulcers resulting from advanced chronic venous insufficiency, leg swelling, not treated varicose veins, it is a standard to conduct a multidirectional model of treatment comprising of:
- local treatment of the wound – treatment by means of dressings,
- compression therapy – treatment with special bandages or stockings,
- drug therapy – treatment with pharmaceuticals – medicines,
- and ultimately the elimination of venous reflux – surgical treatment.
The local treatment is to accelerate the cleansing of the ulcer from necrotic tissue and stimulation of the healing process. The purpose of the conservative treatment is to reverse the effects of venous hypertension, improving venous return, and thus – reducing the swelling. The basis of the conservative treatment is the compression therapy. It increases local hydrostatic pressure and reduces pressure in superficial veins, reducing the transudation of fluid from the blood. Gradual compression accelerates blood flow in the veins of the deep system. An extremely important element of the conservative treatment is the pharmacotherapy.
The treatment of leg ulcers is tough and long-lasting, so to make it the least expensive and effective it must be based on genuine and systematic cooperation with a healthcare professional.
Prevention
Factors which a person can control are WEIGHT and LIFESTYLE.
WEIGHT:
- losing excess weight
LIFESTYLE:
- increasing physical activity especially walking, cycling, swimming. This activities the so-called “calf pump”. Muscle contractions stimulate the venous circulation, pushing blood to the heart – blood does not stop in the veins.
- taking care of yourself in the workplace, especially when staying seated – footrests, avoid staying long in one position without moving or standing. Involving exercises allowing the calf muscles to work – for example, march in place in an upright position, bending towards the foot being in a sitting position.
Once microcirculatory disturbances occur, they can be corrected through the use of compression products:
- knee-socks
- stockings
- anti-varicose tights
and involve medical treatment – always preceded by consultation with your doctor or a pharmacist.
Caroline Burger
Leiderdorp Hospital, the Netherlands
Saving time, cost control and attention to the quality of care – are key elements for the managers evaluating processes in hospitals. One of these processes is the management of widely understood dressing materials. The solution used in the Leiderdorp Hospital in the Netherlands are so called “custom made” sterile procedure sets. The hospital has used that system for many years.
One of the elements to improve work efficiency in the operating suite is the application of “custom-made” sterile procedure sets, which include all disposable materials needed to perform the surgery, in particular: OP-drapes, gowns, absorbent products and a scalpel. It happens that some special procedures need to be also supplemented with different accessories.

Using a procedure set has many advantages.
- Using procedure sets may contribute to standardise the action mode during an operation. A multidisciplinary team (medical specialists, purchase department, logistics department and manufacturer’s product specialist) determine the optimal composition of the set. When the operating procedure gets standardised, it is easier to coordinate the planning of raw materials according to the action plan in the operating room. In this way, the hospital can effectively manage the inventory, monitor the consumption (which must be compatible with the quantity of performed procedures) and thus reduce costs.
- The use of procedure sets can simplify work for the surgical team. This is important for safety reasons, especially in an emergency, when every minute counts, and the time saving can decide about the patient’s life. It is also important for economic reasons: the possibility to perform procedures in a shorter time means that the operating room can be used more efficiently.
- The management of single sterile components needed to perform a surgery requires a large amount of work. One should indicate not only the time and effort associated with their collection and preparation for a surgery, but most of all work associated with maintaining stock which is safe for hospital functioning. The logistics associated with the management of individual sterile components is far more complicated than the process of logistics related to the management of ready-to-use sterile procedure sets. The simplification of this process increases epidemiological security simultaneously reducing costs.
- An important aspect in considering the advisability of implementing sterile procedure sets is their price. The supplier of a procedure set – because of the scale of delivery – is able to reduce the purchase price of the components. Consequently, the price at which a hospital buys components from a single source must be smaller than the total price of purchased components from multiple suppliers.
- The implementation of procedure sets can reduce the costs associated with the disposal of packaging, which are the reminiscent of the individual components.
In conclusion, the procedure sets simplify all stages of logistics associated with the supply of the operating room in the widely understood dressing material, enable to monitor their consumption, and consequently lead to lower the costs.
Nurse assisting in surgeries at the hospital in Leiderdorp:
I cannot imagine working without the procedure sets. Earlier preparation for an operation was very time-consuming. We had to complete all sterile products, check them, and open one by one. The procedure sets, which we now use are “tailored” to our needs. The saved time we can devote to the patient or perform additional operations. An important advantage is the stable quality of disposable materials. We use disposable drapes, thus eliminating the problem of dusting in an operational environment. Currently, we use six different procedure sets e.g.: for surgical procedures, for surgery of the head, neck and limbs. The use of these specialised sets to me and my colleagues has only advantages.



Manager of the operating rooms, introducing the system of procedural sets in the hospital in Leiderdorp:
As a manager I am always looking for ways to reduce costs and increase productivity. We have analysed the costs of the application of procedure sets and came to the conclusion that the time gained in the operating room directly translates into financial benefits. In addition, we save since the set price is lower and we keep less inventory. We didn’t act rashly, before the purchase we gathered a group of experts to develop a set of wide range of applications. This team with the supplier developed together several procedure sets. They were tested and then, according to our requirements, were adjusted to our needs. The standardisation of the work of all professionals was necessary to ensure the efficient use and broad application of the sets. For this joint effort and commitment were maximally rewarded. The productivity in the operating room has increased and the sets are used with our full satisfaction.

Nosocomial infections are a major problem in modern medicine, because many times they are mean a failure in the treatment and the emergence of complications. The most common problems associated with infections is the lack of aseptic behaviour in the where a medical procedure is performed, a delay in the diagnosis of infection or improper treatment. For the hospital, it is connected with the fact that all these aspects – prevention, diagnosis and treatment – must be done properly.
More and more hospitals decide to obtain an ISO certificate, which leads to the development of procedures for all phases of patient treatment, the observance of which will reduce the number of infections. Moreover, the awareness of the medical staff of this problem is increasing year by year.
The problem of nosocomial infections is also a challenge for manufacturers of medical devices used in the performance of specific procedures in health care units.
The answer to the security needs of the treatment are Matoset products that combine functionality and economy by intentional combining of dressing material. In other words, the individual Matoset is dedicated to a given medical procedure, and particular elements are arranged in a way forcing to perform activities in a particular sequence in accordance with asepsis principles. The structured arrangement and thoughtful composition translates to security, convenience and time saving.
Interview:
Monika Cerkaska – TZMO Product Manager
Katarzyna Moś – Master in Nursing with a specialisation in epidemiological nursing
M.C. In which situations the use of sterile Matoset sets worked best?
K. M. In our daily practice we use Matoset products mainly in treatment rooms, when we have to perform minor medical procedures, such as suture removal or dressing change. Using the sterile sets I am sure that I have all the necessary materials prepared and within a few moments I am able to perform a minor procedure. The ready-for-use sets are indispensable at the patient’s bedside when transporting the patient and performing a procedure in the treatment room is not possible.
M.C. And what about situations when you need to change the dressing at patient’s home?
K. M. Exactly. The health visitor will surely appreciate the comfort of using the sets. It is always certain that all necessary materials are prepared, and each patient has a sense of individual treatment and safety guarantee since the set is designed specifically for him.
M.C. So it much easier to work with the set?
K. M. Yes, it’s easier because they improve the course of a medical procedures, but also thanks to them the work is a lot safer. The arrangement of particular elements determines the actions to be performed. We cannot omit any items e.g. gloves, which are usually placed at the top, and only after their application it is possible to use other sterile components. This minimises the risk of infection, and this is important both for us and for the patient. The documentation process is facilitated by adhesive labels with information about the product, which can be placed in the patient’s records.
M.C. So can we conclude that the sets guarantee the asepsis regardless of the place of performing the procedure?
K. M. Yes, we can. The patient is not always in a place where it is possible to e.g. securely change a dressing. Matoset enables us to do so, and also reduce the time to prepare for the procedure and facilitate the organisation of the work.
M.C. At the end I have to ask – what about the costs?
K. M. The application of complete sets dedicated for a given procedure eliminates the need to open multiple unit packaging, which directly translates into the cost of the procedure. When you open a few packs it increases the possibility of infection of the sterile material. Besides, using the sets – all the content is deliberately used. The rational use of dressing material certainly reduces the cost of its purchase. In addition, medical staff does not have to devote time to complete the dressings for the procedure. In conclusion, I would like to add a few words about the catheter sets and sets for the disinfection of the surgical field, which will surely work well in emergency rooms, although, of course, not only. In situations where time counts, we are not always able to fully observe aseptic rules, the lack of which – as you know – can lead to complications and the cause of prolonged hospitalisation. A patient who is in a life-threatening situation requires undertaking multiple procedures at the same time. The risk of infection while saving lives is greater than during the planned procedures. Therefore, the use of Matoset in the form of ready-for-use sets, such as the catheter set helps to observe the asepsis. A set that contains all the necessary components including an adequate size catheter, allows for the reduction of unnecessary actions to a minimum. The same is true also in the case of the set for disinfecting surgical field, which is justified and fully used up when performing medical procedures in life-threatening conditions. During a resuscitation it is often necessary to apply an endovascular electrode or perform a subclavian vein puncture. Having the complete disinfection set we can take care of the proper preparation of the patient for such procedures in a short time. It is important to save a patient without putting him at any additional risk that after a successful resuscitation may lead to an unwanted contamination. We save the patient and instead “give” him an infection and extended hospital stay. The state of emergency passes, and the patient will require treatment for complications resulting from non-compliance with the basic aseptic principles, the observance of which is certainly facilitated by the Matoset.
M.C. Thank you very much for your time.
Working in the treatment room is fraught with high risk of infection, which can be caused in various ways. One of them may be bacterial contamination of instruments, equipment and surfaces used in the course of the procedure. The danger in particular way may relate to the equipment which penetrates into sterile body space. To prevent the spread of infections, it should be ensured that the used instruments are sterile. This requirement applies to all instruments used in the procedures connected with tissue discontinuity, or requiring contact with the mucous membranes or damaged skin, e.g. dressing change or removal or application of sutures. In a situation where re-usable instruments are applied, we are forced to make costly sterilisation process to prepare them for reuse.
Another type of problem is secure collection of infected waste generated during the procedure. Due to epidemiological reasons we are forced to keep them in specially designated containers in accordance with accepted for this type of material rules. In particular sharp instruments should be disposed of with great caution.
A great help in simple procedures is the use of ready-made sets dedicated to perform a specific medical procedure. The set content and their form enables to easily conduct the procedure at any time preserving all security regimes relating to both the procedure itself and the safe storage of contaminated material generated during the procedure.
The advantage of the sets is the safe way to store all the needed materials and their readiness to be used at any time.
The photos present an example of a suture removal procedure with the application of a special dedicated set.
Disposable metal instruments are hazardous waste with sharp ends and edges which are to be collected in durable containers, resistant to moisture and chemicals, with the possibility of single closure.
SET COMPONENTS

COURSE OF THE PROCEDURE




Miroslav Hricišák, MD
A doctor in charge of a same-day medical care unit
Euromedix a.s., ProCare Polyclinic
Betliarska 17, Bratislava
Over the 21 years of my surgical, outpatient care and operating practice, I have worked in many places and there I developed certain work routines and the habit of using proven procedures. As time went on and my experience grew, I worked to improve the procedures, switching to less complicated and more cost-effective working methods whether in outpatient surgery departments or in operating theatres.
After leaving my previous employer, I took on the challenge of building a new outpatient surgery department at the polyclinic and a same-day medical care department specialising in surgery and orthopaedics and, some time later, gynaecology, plastic surgery, urology, and head and neck surgery.
At first I thought that the work would be fairly easy and that I would be able to make use of what I already knew or would learn, and that all other things would come easily somehow.
 The first step was, together with my team, to decide what products we would need. After that, we contacted a number of suppliers to share our ideas and requirements with them. There were, of course, certain limitations, such as the space at the polyclinic premises, a tight budget, the scope of activity or logistics, I had to change my point of view and, in the setup process, make use of many established procedures and routines. My ambition was to develop a model as simple and cost-effective as possible.
The first step was, together with my team, to decide what products we would need. After that, we contacted a number of suppliers to share our ideas and requirements with them. There were, of course, certain limitations, such as the space at the polyclinic premises, a tight budget, the scope of activity or logistics, I had to change my point of view and, in the setup process, make use of many established procedures and routines. My ambition was to develop a model as simple and cost-effective as possible.
One of the key decisions relating to the operating theatres was the choice of OP-drapes. Should we use a laundry or go for disposable surgical drapes and linen ?
In the outpatient surgery department, I tried the small disposable operative sets made by TZMO SA. At first, I was sceptical about using materials that were new to me and that I had never used before. After some time, however, the outpatient operative dressing sets, the tissue sample collection sets or catheter placement sets became my favourite products. The preparations for surgical procedures and the procedures themselves took much less time now.
At the same-day medical care unit, I used different operative sets made by TZMO S.A. specifically for different surgical and orthopaedic procedures. After many surgical consultations and discussions with TZMO S.A., the manufacturer provided us with “made-to-fit”, large operative sets containing sterile disposable OP-drapes, such as patient drapes, instrument table covers and surgical gowns. We also ordered some accessories, which were also made and packed on a custom order basis. The sets contained sterile items, such as different dressings, bags, self-adhesive pockets for liquids and medical equipment, plus tampons, bowls and elastic bandages.
The operative sets also contained disposable metal instruments (scissors, tweezers etc.), but I haven’t been using these instruments for long enough to say what I think of them.
We liked the operative sets supplied by TZMO SA so much that after three months of working in the same-day medical care unit, we discontinued using materials from other suppliers.
Being a small team, we are doing our best to perform the largest possible number of surgical procedures in the shortest possible time. Large operative sets help us reduce the time needed to prepare our operating theatres for procedures. Also, when we need to replace our surgical nurses with external surgical personnel, the risk of failure due to different working habits is none. The large operative sets designed for specific surgical procedures have made our work easier and improved the safety of our patients and our personnel.
The operative sets also contained disposable metal instruments (scissors, tweezers etc.), but I haven’t been using these instruments for long enough to say what I think of them.
We liked the operative sets supplied by TZMO SA so much that after three months of working in the same-day medical care unit, we discontinued using materials from other suppliers.
Being a small team, we are doing our best to perform the largest possible number of surgical procedures in the shortest possible time. Large operative sets help us reduce the time needed to prepare our operating theatres for procedures. Also, when we need to replace our surgical nurses with external surgical personnel, the risk of failure due to different working habits is none. The large operative sets designed for specific surgical procedures have made our work easier and improved the safety of our patients and our personnel.

With standardised surgical procedures, the risk of errors and, consequently, the possible complications is reduced. The post-surgery cleaning and material removal jobs are now much easier, which gives us more time to prepare for the procedures that follow. The central sterile services department personnel no longer have to sterilise surgical materials, as these are supplied sterile by the manufacturer. As a result, the surgical nurses can focus on the surgery itself. The standardisation of procedures through the use of large operative sets offers economic benefits too. Normally one set is used during one surgical procedure, meaning that there is practically no waste (unused materials). Keeping records of the use of the materials is easy – the material labels with codes are inserted in the files for archiving. This helps to calculate the actual costs of procedures. The costs of the personnel involved in the storage and processing of surgical materials are also reduced.
After my experience of using small and large operative sets at the polyclinic and the same-day medical care unit, I would never switch to other solutions.
The word ”end” means not just the end, but also the goal. In Polish the ”end” is rarely used as the goal, and more can be associated with the closure of one stage and the start of a new and different one from the current reality. Thinking straight the end is a new beginning i.e. changes.
Changes are often associated with fear and temporary difficulties, which people are not always ready for. The need to leave the safe and tame zone always causes fear of what will happen.
If the proceedings are recorded in the medical procedure, the change of this action seems to be very difficult and unreasonable, because the current performance of procedures was effective and unchanged for many years. However, it often happens that the change involves a number of positive consequences, and thus modification of the previously stable reality in a very positive way.
The effects of changes associated with the introduction of ready-for-use-sets and the benefits resulting from that are discussed by:
Emilia Zawadzka
Master of Nursing with specialisation in epidemiological nursing – Dr. Władyslaw Biegański Regional Specialist Hospital in Grudziądz
Monika Cerkaska
MatoNews interviewer
Monika Cerkaska: Why did you decide to work with specialist sets? Is it only because of the relief for the Central Strerilisation Unit?
 Emilia Zawadzka: From the moment the CSU started to support 11 operating rooms, we decided to use it only for the sterilisation of instruments. Relieving the work of CSU we resigned from creating sets of dressings material inside the hospital and decided to use sterile procedure and operative sets. I am thinking of ready-for-use sterile products, in a single package containing both the dressing material, Op-drapes and other components needed to perform a particular procedure. In this way the responsibility for the sterility of the material is transferred onto the manufacturer, and the CSU can focus on the preparation of sterile surgical instruments.
Emilia Zawadzka: From the moment the CSU started to support 11 operating rooms, we decided to use it only for the sterilisation of instruments. Relieving the work of CSU we resigned from creating sets of dressings material inside the hospital and decided to use sterile procedure and operative sets. I am thinking of ready-for-use sterile products, in a single package containing both the dressing material, Op-drapes and other components needed to perform a particular procedure. In this way the responsibility for the sterility of the material is transferred onto the manufacturer, and the CSU can focus on the preparation of sterile surgical instruments.
Due to such a decision, a large work load relief was also felt by nurses who were expected so far to prepare sets of dressing material. Not only the work comfort increased, but also ensured our and patients’ safety. The use one set specifically designed for a given surgical procedure eliminates the risk of error and thus minimises the risk of complications. In addition, the time devoted to prepare all the necessary materials for the surgery is much shorter, which is especially important in life-saving situations.
The use one set specifically designed for a given surgical procedure eliminates the risk of error and thus minimises the risk of complications.

M.C.: What kind of response from the doctors and nurses, the direct users of the sets, did you meet while changing into ready-for-use sets?
E.Z.: Any change or introduction of a new solution causes some concern among those who are directly affected. So it was in our case. Both among the doctors and nurses there were concerns that quickly disappeared when they started working with the sets. We all experienced better working conditions, and today we cannot imagine return to the previous state. It is much easier and safer to open one set than a few products in aseptic packages. While opening one package, we reduce the possibility of contamination of products and patients with pathogenic microorganisms. In high-risk procedures with high risk of complications the elimination of errors translates into patient’s safety, which is the most important thing for us.
M.C.: Which elements of the set are the most important for you?
E.Z.: First of all, the set should be complete, but not exaggerated. Unused elements constitute waste, for which, unfortunately, you would need to pay. Therefore, the most important are the basic elements, which if necessary can be supplemented with sterile material. In an emergency, when there is time pressure, it is important that the set contains everything necessary to carry out the procedure.
An important advantage of the product in the form of the set is the fact that the order of arrangement of individual elements can enforce the execution of particular activities, e.g. first the instrument table is covered, the OP-field is disinfected and secured in the right way. These are the activities which are always followed one another, and the order in which they appear has a big impact on the safety of the procedure.
M.C.: What about human habits? Do they not induce resistance to the use of medical devices in such a form?
E.Z.: The procedure should be carried out in a safe manner and habits should most of all provide the security. I do not see any conflict of interest.
Speaking of safety one must also think about legal security when a patient can claim against the hospital, like in the case of medical incidents. The awareness of patients is increasing, the affairs between the patient and the hospital quickly become media events, and each won process generates another claim. Therefore, it is important to have evidence that all the procedures in the treatment of the patient are carried out in a secure way. Medical records are proof in this case, which are facilitated by a TAG label i.e. stickers that can be stuck into the patient’s medical history and the documentation of the operating theatre.
M.C.: Which arguments do you think are stressed by the hospital manager?
E.Z.: I’m sure that epidemiological safety and costs. The cost reduction and of course the set price is very important, and for the director / manager the transparency of costs. The set price is equal to the real cost for the ward for the performed procedure. We are talking about a simple ratio: the number of sets is equal to the number of performed procedures. In this case we eliminate the so-called hidden costs and limit the possibility of manipulation of the costs of individual procedures.
M.C.: The economic aspect is a very strong argument. What about work ergonomics in the ward? Is it changing?
E.Z.: Of course. It great relief is felt by the personnel. Workload for nurses is very high, and in a situation where we use ready-made sets, all the energy is focused on the patient.
In addition, the use of sets streamlines logistics inside the hospital. Products are transported easier and safer.
M.C.: Thank you very much for your time.
Dr. Władyslaw Biegański Regional Specialist Hospital in Grudziądz has 40 wards, in which there are 1,050 beds and 53 specialised outpatient clinics. Modern operating theatre has 11 operating rooms supported by a Central Sterilisation Unit (CSU). Due to the large relief for the functioning of the CSU the hospital has completely changed the approach to purchase management of products for the greater use of ready-made sterile procedure and operative sets and the transition from reusable to disposable products.
Within the European Regional Development Fund the hospital acquired also funding for the purchase of new ambulances with equipment, for the construction of one of the most modern heliports in Poland and for a wide range of medical equipment that is used in the treatment of patients in the new clinic.
The use of large operative sets in the operating theatre of the Nicolaus Copernicus Provincial Specialist Hospital in Łódź are discussed by:
Sylwia Dąbrowska
Deputy Head of the Operating Theatre for Nursing – Nicolaus Copernicus Provincial Specialist Hospital in Łódź
Monika Cerkaska
MatoNews interviewer
Monika Cerkaska.: What urged you to start working with ready-made sets?
Sylwia Dąbrowska: The decision to introduce the standard use of disposable sets in the operating theatre happily coincided with the renovation of the operating theatre. Once, that is before the renovation, within the operating theatre we had a sterilisation unit, where in addition to current work for the needs of the theatre, there were also sets of non sterile materials prepared that in the next step were sterilised. After the renovation of the operating theatre, the sterilisation unit was closed and today the hospital has only a delivery and receipt point dealing with logistics, mainly of instruments and hospital clothing. Due to such a decision at one time we started to use disposable products such as surgical drapes, gowns and procedure or operative sets.
The renovation of the operating suite also reduced the size of storage space that we have. Therefore, we cannot afford to maintain a very large stock of non sterile products, which always occupied a lot of space. Nowadays, we use a very large number of implants, and they mainly take place in the operating room. Dressing materials are stored outside the operating room, and therefore it is easier and safer then to use a ready set. Such an organisational approach is very reasonable. Reducing the storage space, the space for the patient increases. And this is of course connected with money.
One move is enough to open the set, one set designed for a given procedure, and one label that allows the transfer of information to the documentation highly limit the time devoted to prepare for a surgery. This allows the medical staff to concentrate on their work around the patient.

M.C.: You mentioned the safety. It’s probably one of the most important reasons for the hospital, for which you have decided to work with the ready-for-use product?
S.D.: Of course, and it is for the hospital as a whole. This is a very strong argument for the manager – because the responsibility for sterility lies with the manufacturer – and for the entire epidemiological staff – for the use of sets reduces the number of hospital-acquired infections. It is also very important for us – as the medical staff. It is safer to open one packaging rather than opening individual packages of products needed to complete the procedure. The removable part of the label is a very safe element. To eliminate the error, which can be committed in the process of rewriting the data into the documentation, in this case only one sticker with a product code and expiration date is transferred. The product code fully identifies the contents of the package and there is no need for a more detailed label. At the big amount of material used and also having a limited amount of place in the documentation, the size label is adequate.
Another advantage of using the sets is to increase work comfort. One move is enough to open the set, one set designed for a given procedure, and one label that allows the transfer of information to the documentation highly limit the time devoted to prepare for a surgery. This allows the medical staff to concentrate on their work around the patient This is especially important in a situation where for example on call there are three operating rooms functioning, and there is just an enough number of nurses to do the work on the ward. Using the finished product allows for smooth work throughout the operating suite on duty. Of course, the comfort of using the sets is experienced not only in emergency situations, but also in our daily work. We minimise the duration of the procedure, which translates into individual savings, i.e.: lower consumption of energy and air conditioners, shorter anaesthesia, shorter work of a surgeon, anaesthetist and nurses. Minimising the time devoted to the preparation for a surgery, combined with efficient team work makes the performance of the procedure faster and cheaper.
M.C.: The cost is still to be discussed, but yet another question arises. Do I understand it correctly that the work with the sets increases the efficiency of the operating room?
S.D.: By all means yes. In addition to the mentioned sets also the high quality of disinfectants that allow for very rapid turnover of patients in the operating room contributes to better efficiency. Taking our hospital into consideration, I can say that until recently, daily we performed four procedures e.g. strumectomy. Today we can perform five operations and we have still some reserve time. This shows the efficiency and getting in sync of the team, as well as shorter time devoted to prepare for a surgery. This is most noticeable while analysing the productivity of the operating suite for a month or a year.
M.C.: Yet another question about the waste. Can we assume that the amount of waste gets reduced?
S.D.: It depends. Generally, the amount of medical waste coming from the operating theatre increases. This happens in all medical units using disposable products like disposable OP-drapes, medical devices, gowns, etc. However, the amount of waste, in the case of unit packages of the products used during the treatment certainly drops and is limited to a few, and not as it once was – a dozen or even dozens.
M.C.: So how do the costs of a procedure change after implementing disposable ready-for-use sets?
S.D.: I have no doubt that this solution is far more profitable for the hospital, because we have a finished and adjusted for our needs set, sterilised and delivered. Completing components inside the hospital in our reality would involve an additional job position, and that means an increase of the cost of the procedure. The best and the most advanced solution are sets dedicated for a particular medical procedure. This reduces not only the amount we opened dressing materials, but also in such sets you can find OP-drapes, a Mayo table cover, covers for equipment and cables, organisers for the equipment used during a surgery – a very useful and work ordering thing i.e. a whole load of sterile material. In this case, the cost of the given procedure is countable and very readable. The number of performed procedures is equal to the amount of used sets.
M.C.: Thank you very much for your time.
Nicolaus Copernicus Provincial Specialist Hospital in Łódź in its complex structure has: Specialist Hospital, Regional Oncology Centre, Dr. Janusz Korczak Paediatric Centre, Group of Clinics and Specialist Clinics as well as Diagnostic Department.
The biggest success for the hospital was the creation of the Bone Marrow Transplant Centre managed by a specialised team of experienced scientific and technical staff, and the creation of a Hospital Emergency Department integrated with a heliport forming a functional unit guaranteeing rapid rescue in life threatening situations. An important achievement was the modernisation of the Regional Oncology Centre.
Currently, the hospital provides comprehensive diagnosis and treatment at the highest level, thus providing conditions for faster patients’ recovery.
In the hospital there are also 12 associations and foundations supporting inter alia patients with cancer, leukaemia, haemophilia, rheumatic diseases, a heart transplant, and many others.
Anna Rogalewska, Patrycja Judycka
Toruńskie Zakłady Materiałów Opatrunkowych SA
Evolving trends in wound dressing
From herbs and leaves, to gauze and bandage, to professional dressings, the practice of wound dressing has been evolving for tens of thousands of years. For over 60 years, Toruńskie Zakłady Materiałów Opatrunkowych (TZMO) has been delivering trend-setting products in wound dressing. Over the years, we have made changes to our range of dressings and the way we make them, but one thing has been constant: we continue to take care to deliver top-quality products that meet the most rigorous safety standards. TZMO’s Matopat-branded medical products have always been a symbol of high quality, innovation and biocompatibility.
Choosing the right dressing: What should patients take into account?
First of all, it’s the kind of wound, as different wounds heal differently. You will need a different dressing for a surgical wound, or incision (such wounds must be dressed precisely, in a sterile manner, by qualified medical personnel in a suitable place), a different one for a new post-injury wound and a yet different one for a difficult-to-heal wound with substantial tissue loss. Once you have identified the kind of wound you’re dealing with, you need a professional dressing that will not only reduce the risk of infection and offer optimal healing time and effectiveness, but also help the patient feel more comfortable. There has been a noticeable trend in the use of professional wound dressings: in the past, they were used only by medical professionals in hospitals, but now they are making their way to pharmacies. As a result, professional wound dressings can today be used by patients at home.
The properties of professional wound dressings
For a small cut or chafe, a clean and comfortable sticking plaster will do the job. Apply it to the affected area and leave it for a scab to form and the wound to heal. However, in the case of more serious wounds, such as surgical wounds, it is advisable to use professional dressings such as those used in hospitals. Professional surgical dressings are sterile, absorptive and flexible, and designed so that the adhesive can keep the dressing tight on the affected area, preventing dirt or other unwanted matter from penetrating the wound. At the same time, the absorption material should be sufficiently protected to prevent direct contact of the dressing with the surface of the wound or with the surgical sutures. Professional dressings are also air-permeable to allow the skin to “breathe”.
 Examples of professional dressings for surgical wounds include Fixopore S and Fixopore F. The former is made of flexible, nonwoven fabric that easily fits in even hard-to-access areas of the patient’s body and will not limit the patient’s movement. A nonwoven fabric dressing is the basic type of dressing used by hospitals for surgical wounds. This dressing has a special, smooth layer of absorption material that will not get stuck on the wound or suture, thus allowing for safe and painless dressing changes without the risk of damage to the absorption material. The adhesive on the dressing is hypoallergenic. The other of the two products, Fixopore F, is made of ultra-thin polyurethane film that keeps moisture away from the wound. This helps patients to go about their regular daily activities without having to change their dressings frequently and without the risk of infecting the wound. The benefits of modern wound dressings can be enjoyed fully if the dressings are used in accordance with the user’s instructions.
Examples of professional dressings for surgical wounds include Fixopore S and Fixopore F. The former is made of flexible, nonwoven fabric that easily fits in even hard-to-access areas of the patient’s body and will not limit the patient’s movement. A nonwoven fabric dressing is the basic type of dressing used by hospitals for surgical wounds. This dressing has a special, smooth layer of absorption material that will not get stuck on the wound or suture, thus allowing for safe and painless dressing changes without the risk of damage to the absorption material. The adhesive on the dressing is hypoallergenic. The other of the two products, Fixopore F, is made of ultra-thin polyurethane film that keeps moisture away from the wound. This helps patients to go about their regular daily activities without having to change their dressings frequently and without the risk of infecting the wound. The benefits of modern wound dressings can be enjoyed fully if the dressings are used in accordance with the user’s instructions.
Educating patients
A pharmacist’s role is not only to help patients choose the right dressing, but also to educate them about the need for taking proper care of their wounds. Wound cleaning and correct dressing changes are essential and, apart from the choice of dressing, will help the wound to heal quickly and without complications. A general rule in professional wound healing is that dressing changes should be as rare as possible, following the recommended dressing use time, and as frequent as possible, depending on the appearance of the wound and the condition of the dressing.
For more information about professional dressings for different wound types, please visit: en.matopat-global.com
Bożena Krymska
Specialist for epidemiological and cardiac nursing – Silesian Centre for Heart Diseases in Zabrze
The quality of medical services means meeting or surpassing the expectations of the patient, the compliance with standards and the degree of realising the benchmarks. According to H. Lenartowicz high-quality health care is one that corresponds to certain criteria, indicating compliance with current professional knowledge and that which, under given circumstances, enables the patients to achieve desired health results. The quality of offered medical services is very important because it concerns the priceless value of life and health of the people making use it.

Although the quality is in fact the satisfaction with well performed medical services, for each party – the performer and the recipient of the service – it means something else.
- For the patient, the quality of medical services depends on the efficient recovery or health improvement after leaving the hospital.
- For employee of the health care facility, the quality is understood as the compatibility of this service with current professional knowledge and achieving health improvement without adverse events.
- For the management of the facility, the quality is to provide services at a sufficiently high level with a correspondingly lower cost.
Any medical procedure performed in a patient comprises several steps:
- preparation of a set,
- performing medical actions,
- disposal of the set, waste management,
- documenting the procedure,
- preparing equipment and reusable instruments for reuse.
Each of these steps requires effort, resources and time. Performing the procedure under various conditions, especially in rapid situations and in emergency rooms, is at high risk of error, which can undoubtedly affect the quality of the procedure, and therefore the quality of the overall medical service.
All of the above steps can be improved by ready-for-use sets adjusted for different procedures and medical treatments. The preparation of a “traditional” set includes the completion of an appropriate amount of equipment, instruments, medicines, and dressing material needed to perform the procedure. However, a ready-for-use set saves the preparation time, especially if the particular procedure is performed urgently. The nurse does not have to wonder how many items to prepare and what exactly is needed. The set provides materials needed to carry out the procedure in terms of their quality and quantity.
The content of the final set forces to perform the procedure in one correct way without omitting certain activities. An example would be the optimum number of six gauze tampons included in the set for bladder catheterisation, which demands to devote enough time to disinfect the area surrounding the urethral meatus, if all the tampons are used. The outer package in form of a rigid blister, often with a few chambers, may serve as a container for liquids or waste material, eliminating the need for additional vessels.
The ready-for-use allow to perform a procedure, opening only one sterile package, which greatly reduces the amount of waste, e.g. many external packaging of: sterile swabs, instruments, gloves, syringes, etc. The sets are completed optimally for a given procedure, which means that any such intervention is carried out using the same amount of equipment and dressing material. In practice, when we complete a set ourselves, there is often a tendency to open more packaging of e.g. dressing material than needed (swabs, cotton balls), just in case, in order not to run out.
The procedure performed using a ready-for-use set quickly becomes standardised, enables to easily monitor the consumption of materials, and thus counting the cost.
It is very easy to clean after the procedure. Everything that has been used is one medical waste. In view of the fact that everything in the set is disposable, the entire material is directed to the waste, without the need to segregate.
It is very simple and accurate to document the performed procedure due to the included self-adhesive labels.
The use of disposable instruments included in the set brings savings, resulting from the elimination of further re-sterilisation. The sterilisation process means additional costs: water, electricity, disinfecting agents, sterilisation packaging, , sterilisation tests, and human effort.
One of the major advantages of the sets is the elimination of adverse events, such as the prevention of infections. Returning to the quality of medical services, the implementation of a program to prevent hospital infections, and systemic efforts to prevent errors in medical procedures is very important to ensure high quality. Reducing the number of infections is an objective indicator of the quality of medical services, and any infection that occurred, and which could have been avoided, is a failure of the institution providing health services. The ready-for-use sets “tailored” to a specific procedure are a perfect tool to prevent such failures. The sets guarantee the sterility of equipment and materials used to perform the procedure. Therefore, the manufacturer takes the responsibility for their sterility, and thus for the quality of the medical device.
Undoubtedly, the application of the sets in practice improves work, gives satisfaction to medical staff, reduces costs, and leads to patient satisfaction. Moreover, better quality of medical care leads to the increased competitiveness of the medical facility in the market.
Literature
- Ciuruś M., Hygiene procedures in health care facilities, Institute for Health Protection, Warsaw 2009.
- Dykowska G., Opolski J., The quality of health care services, self-education package, Warsaw 2001.
- Heczko PB Wójkowska-Mach J. (red.), Hospital infections. Handbook for infection control teams, PZWL, Warsaw 2009.
- Holub, J., Competitive quality strategy on the medical service market, [in:] Nogalski B., Rybicki J. (red.), Modern management of a health care facility, Dom Organizatora, Toruń 2002.
- Lenartowicz H., Quality management in nursing, CEM, Warsaw 1998.
- Maciag A. Kruszewski, K., Topczewska-Tylińska K., Michalak J., The Role of processes, standards and procedures in shaping the quality of health services, Alfa-medica Press, Bielsko-Biala, 2007.
- Piątek, A. Improving the quality of nursing care [in] Ksykiewicz-Dorota A. (red.), Fundamentals of organising nursing care, published by Czelej, Lublin 2004.
Yearly about 1% of our population gets burned. The number of Poles affected by burn injuries reaches even 400,000 patients a year. Mostly 50-80% of the burned are children in the 2-4-year-old age group.
Burns can be divided by depth:

- 1st degree – a superficial burn. Only the surface layers of the skin are affected. The symptoms include redness (erythema) and painfulness. The wound usually heals without any complications and scars.
- 2nd A degree – extends into superficial (papillary) dermis. Those wounds are usually very red with clear blisters and are extremely painful. After 2nd A injuries there might appear small discolorations or even scars.
- 2nd B degree – extends into deep (reticular) dermis. In those type of burns superficial epidermal and dermal necrosis might appear. Those wounds are very painful, without blisters, pale or pinkish, grey, bricky or even black. Moreover, they may leave nasty hypertrophied scars.
- 3rd degree – extends through entire dermis. These wounds are usually russet, brown, pale yellow or red.
- 4th degree – extends through skin, subcutaneous tissue and into underlying muscles, tendons, bones, joints.
In the 3rd and 4th degree burns the skin reproductive layer is impaired or completely damaged.
Complications of burns
Quite a frequent complication of burns are hypertrophied scars and joint contractures. The hypertrophied scars appear, among other things, as a result of the increase in blood flow, fibroblast development and collagen deposition as well as of chronic oedema. In all those cases, when strong redness of the scar does not disappear up to two months, and the scar gets thicker and thicker, a keloid scar is very likely to develop. Keloids have a lumpy structure, which is a result of increased metabolism. Their growth is stimulated by microphages and fibroblasts, evoking an overgrowth of collagen fibres. Those complications are inconvenient because they delimit the functioning of the motor apparatus and at the same time they blemish the affected person.
Prophylactically appropriate positioning of the body and joint immobilisation by means of splints or orthopaedic devices is practised. It has also been proven that the application of constant pressure, increasing the capillary pressure of vessels i.e. about 25-30 mmHg, has a beneficial influence on scar formation, and prevents the overgrowth to a large extent. A long-lasting pressure causes an oxygen deficiency in tissues, a deceleration in metabolism and a fibroblast reduction. An increase in the activity of a collagen-decomposing enzyme (collagenase) results in a visible scar reduction.
The pressure method in supporting the post-burn scar treatment has been worldwide known for many years, and it is also commonly used in Poland. The pressotherapy is found to be the most effective method, though there are many alternative ones such as laser therapy, kriotherapy etc.
Apart from negative health effects, quite often the keloids are also harmful to patients’ mental state, resulting sometimes in social exclusion. In modern techniques, and medical procedures it is clearly stated that an effective post-burn rehabilitation needs to be designed in such a way to reduce the keloid formation. An important element of modern treatment support techniques is the application of compression combined with the activity of silicone dressings like e.g. CodosilTM ADHESIVE.
Mechanism of post-burn scar formation
Every wound has the possibility of self-healing. Superficial wounds, in which the topmost layer of the skin (the epidermis) is scraped off, heal without leaving any scars. At the beginning of the healing process the wound is cleansed, so there appear a lot of macrophages and histiocytes. The neoformation of capillaries is evoked, facilitating the appearance of multipotent cells – lymphocytes, which have the ability to turn into fibroblasts. A fibroblast is a type of a cell that synthesises the macromolecules building connective tissue. This cell synthesises tropocollagen, which by polymerisation creates collagen fibres. As those fibres get created, the involution of capillaries takes place, the activity of fibroblasts is lost, and the reepithalisation process is initiated.
In burns, when the epidermis, the papillary layer and the reticular layer get damaged, a stronger hyperplasia of vessels is observed. The widening of vessels, and the appearance of anastomoses causes blood to stop in the healing place, and provides a good access to nutrients; a lot of highly active fibroblasts appear as a result of the production of a great number of collagen fibres.
The reconstruction along with the scar formation takes place at the newly created fibroblasts’ expense, where gradually myofibroblasts – responsible for contractility – get distinguished, while mastocytes take care of the progressive maturation of the scar. Biochemical tests of a scarring process show that there is an increased collagen synthesis in comparison with a normal healing process, and there are also qualitative disorders connected with the increase in the number of mucopolysaccharide matrices, and the decrease in the number of lipids (mainly linolic acid) in the scar. It seems that the reason for this lies in the reduced amount of collagenase (a collagen-decomposing enzyme), resulting from the increase of 1 – antitrypsin and 2 – mucoprotein globulins. Those effects occur probably along with a toxic mitochondrial activity in the damaged cells. This activity takes place in burns from the first moment up to the 10th day of the healing process, when it is possible to notice that those symptoms stop, and a gradual comeback to a normal state, or also an objective steady growth takes place up to the 14th and after the 21st day, if any scarring complications appear.
Moreover, also the effect of the adrenal gland on scar fibroblasts, and their uncontested influence on scarring processes has been recognised. This is the base to examine possible mutual correlations between the prevalence of scarring complications and endocrinological changes in children. Obviously such a correlation takes place during a burn shock, and its further development is not known. Topical scar complications developing after a burn can be either of an aesthetic or of a functional type, or of both types simultaneously. From a histopathological point of view the cicatrical changes are of a hypertrophic, a contractile or a keloid type. Popularly it is said that this happens in 50% of burn cases; however, the factors indicating those changes has not been determined yet. Their impact on the early estimation of an actual scar development possibility is also not known. Especially when it goes about keloids – they are likely to develop even in 80% of places vulnerable to stretching or tension.
Pressotherapy – an effective therapeutic method for post-burn scars
An elastic pressotherapy as a preventive and therapeutic method started to evaluate in the 70s, and turned out to be very effective in supporting the treatment of post-burn complications. This method involves using hypercompression (or just compression) to give constant pressure on keloids. This pressure on the scar gives an ischemic effect, which makes afferent vessels smaller, which results in the reduction of vessel embryos. On one hand, the scar will be supplied with less blood if we reduce the number of blood vessels, but on the other hand, depending on the diameter of the vessel embryos, the blood flow will be increased, and there will be no stasis, which will further influence the reduction of produced collagen fibres, and prevent the wound area from shrinking.
A correctly applied pressotherapy involves the use of strong pressure on the wound after finished epithelisation by means of different types of bandages made of natural latex. Such products are produced of latex threads covered with synthetic fibres.
Their application on the scar and the stable pressure they give can change and improve the content and the quality of various tissue elements. This change in the tissue components results in the qualitative improvement, weakening and decreasing the size of the scar, and at the same time due to the accompanying ischemia, the characteristic red colour of the scar is fading.
General rules for the use of pressotherapy:
- the pressure should be applied as soon as possible (from the moment of wound re-epithelisation, during the next 2-3 years – this is the estimated time for scar development), more or less 1 or 1,5 year;
- constant uninterrupted and long-lasting application of pressure on cicatrical places through an individual adjustment of special compression garments with compression level from 20-25 up to 50 mm Hg/cm2.
To reach the best results it is necessary to observe and control the entire process of the compression rehabilitation, and to change the compression garment periodically since the knitted fabric loses its elasticity, or the patient’s size might change as well.
The time of the compression therapy is varied – optimally up to 2 years. If any topical complications appear such as skin irritation, intertrigo, skin breaks or patient’s psychical inconvenience – the pressotherapy should be temporarily interrupted and then repeated, trying to eliminate those symptoms. [1]
Compression levels in pressotherapy
Compression clothing is characterised by a precisely defined pressure level exerted on the patient’s body. The pressure is expressed in a unit – millimetre of mercury (mmHg). The efficiency depends on the size of the garment, which is to be individually adjusted to a given person after taking precise measures of the patient’s body. The effectiveness of the therapy is also affected by the choice of an appropriate compression level, which depends on the disorder type and its severity. It is highly important to choose the right compression level of a compression product, for too little pressure will bring no effect, and too big pressure can cause many undesirable side effects. The complications may start from very simple ones such as chafes, abrasions or maceration, up to more serious ones such as serous blisters or decubitus ulcers. Those and other side effects resulting from a wrongly chosen compression level, quite often make the patient break the therapy.
The most popularly used compression level classification is the one used in Germany, Switzerland and Italy. In all types of classifications class 1 means the lightest compression, and class 4 the strongest compression. The values express compression given by a product at the ankle joint high. It is important to maintain a compression gradation given on the limb at the entire length of the product. In this case usually there is a rule applied to use 100% compression of the given class (from 1 to 4) at the ankle high (distal part of the product), up to 40% of the compression in the closer (proximal) part.
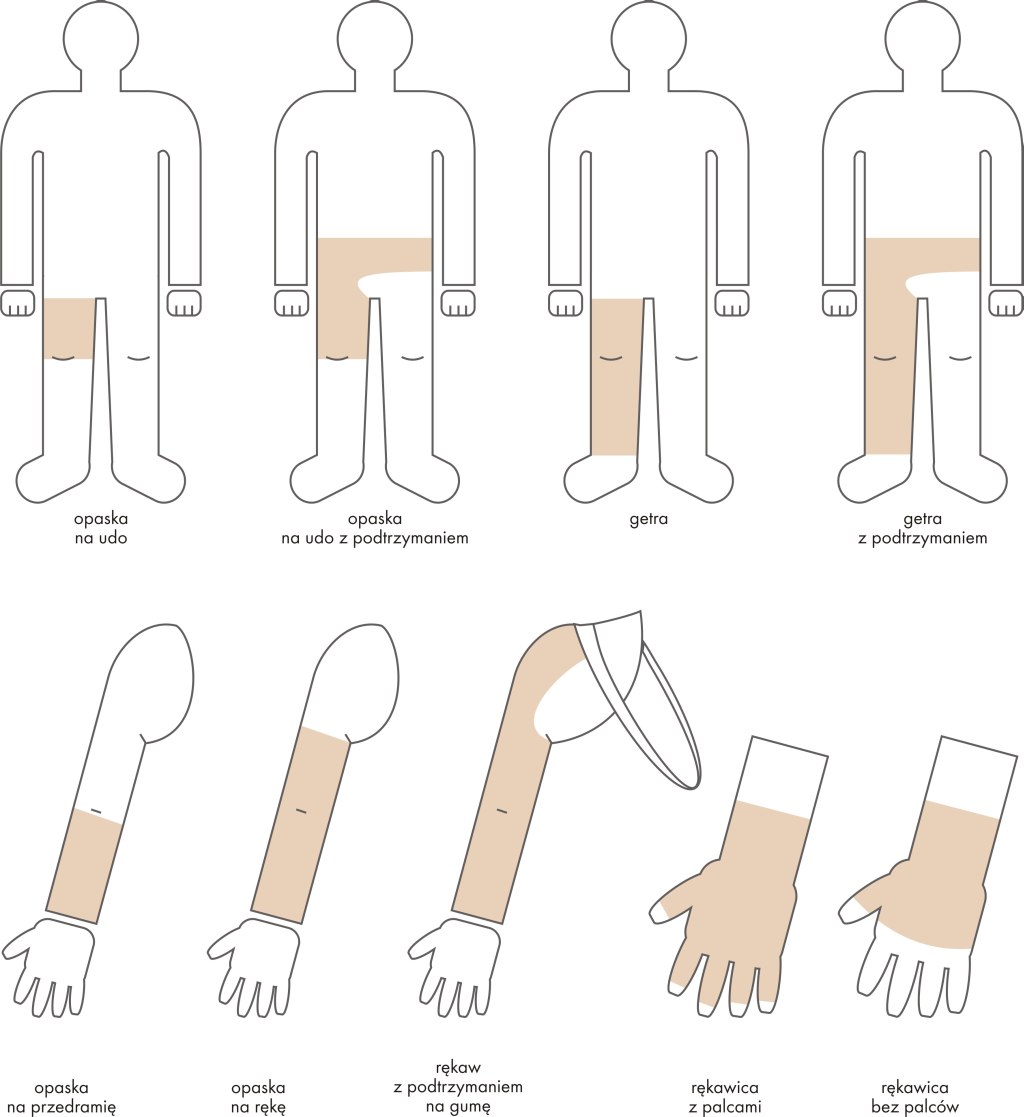
Producers use different classifications of compression; however, the one specified by the European Standardisation Commission distinguishes the following ones:
- class 1 – light compression (18-21 mmHg),
- class 2 – medium compression (23-32 mmHg),
- class 3 – strong compression (34-46 mmHg),
- class 4 – very strong compression (over 49 mmHg).
Efficient therapy with the application of compression garments Codopress®
The success of the therapy highly depends on appropriately chosen compression clothing. Compression garments Codopress® produced in Łódź (Poland) by Tricomed SA are used for supporting the treatment of post-burn scars and in prophylactic rehabilitation of burns. Up till now over 20 thousand products Codopress® have been prepared, successively developing the product range, and improving the construction. The garment is produced of a highly elastic breathable knitted fabric of medical quality, composed of a polyurethane and polyamide yarn. This combination enables to obtain required parameters, and at the same time to provide high comfort for the user.
The manufacturing process makes it possible to produce the garment for every body part according to the compression class recommended by a doctor. The 1st class compression (18-21 mmHg) is the one most frequently used. It is remarkable that all compression products Codopress® are manufactured so that all seams are aside from all scars. Thanks to this the value of the therapeutic pressure is not changed in any way in this place.
The process of compression garment preparation:
- Get a referral from a specialist.
- Make an appointment with a person taking measures of the limb or other body parts.
- Once the garment is sewn it needs to be tried on to make sure that it fits perfectly.
- The patient is trained how to use and clean the product.
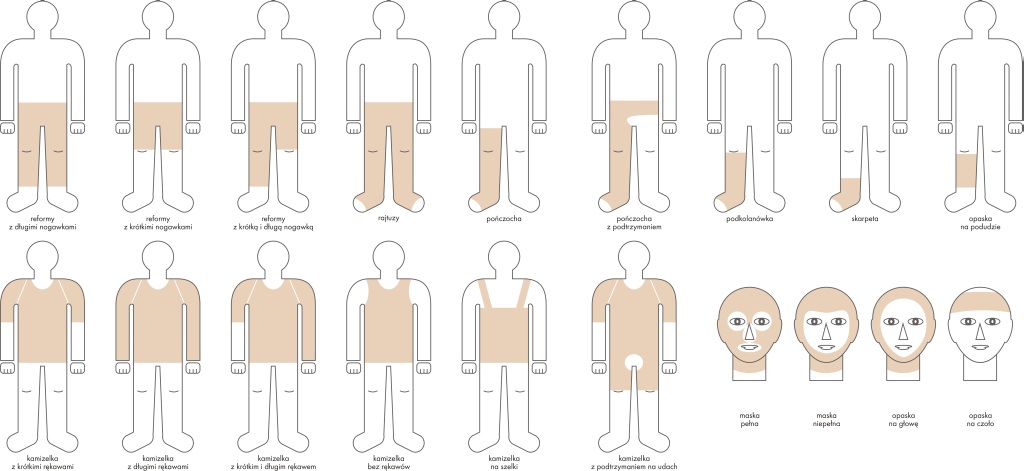
All compression garments should be worn permanently from 6 to 24 months after the wound healing process is finished, till visible rehabilitation effects appear (flattening, fading and softening). The entire therapy usually requires a few changes of the compression garments, along with the use up of the garment and the change of patient’s body size. It is important to remember to use the products only when the post-burn wound is fully healed – see pictures below:


Individually prepared Codopress® products:
- give appropriate compression on the scar,
- can be used with other types of therapy,
- cause no allergic reactions or skin irritations,
- release itching,
- prevent from joint contractures.
Clinical trials
In specialised burn healing centres in Siemianowice (Poland) and Polanica Zdrój (Poland) – leading centres healing heavy burns – a wide range of patients were clinically examined. They tested the effectiveness of Codopress® products in the rehabilitation of post-scar burns.
Clinics testing the Codopress® clothing included the Burn Treatment Ward of the Municipal Hospital No. 2 in Siemianowice Śląskie ran by S. Sakiel, MD, and the Plastic Surgery Hospital in Polanica Zdrój under the supervision of K. Kobus, PhD, Dr h. c. What is more in the National Medicines Institute under the direction of W. Zalewski, PD tests were carried out as for the irritating effect on the skin of the knitted textile used in the production of Codopress® products.
Materials and methods
Within 2 years compression products produced by Tricomed SA were tested in 40 patients at the age of 2 to 59 years old with the average burn area of 26%, and deep burns at the entire skin depth with the average area of 9%.
The patients were divided into two groups:
- in the first group (20 patients) the compression products were applied right after the wound was healed,
- in the second group (20 patients) the Codopress® products were applied after about 3 months after the wound was healed.
The evaluation concerned the face, the neck, the chest, the upper and lower limbs. Overall in the first group 24 places and in the second group 30 places were observed.
 The tested products were evaluated as for their usefulness in supporting the treatment of hypertrophied scars and keloids in 26 patients aged 3 to 58 years. Most of the hypertrophied scars and keloids were caused by hot fluids or fire. The entire healing period for a burn wound, starting from the application of the compression products, took a month up to 4 years. Before the application of pressotherapy, massages were applied. Body parts that were most often tested as for the usefulness of the compression products included: the knee and elbow joint, the buttocks, the hips, the shoulders, the chest, the upper and lower limbs.
The tested products were evaluated as for their usefulness in supporting the treatment of hypertrophied scars and keloids in 26 patients aged 3 to 58 years. Most of the hypertrophied scars and keloids were caused by hot fluids or fire. The entire healing period for a burn wound, starting from the application of the compression products, took a month up to 4 years. Before the application of pressotherapy, massages were applied. Body parts that were most often tested as for the usefulness of the compression products included: the knee and elbow joint, the buttocks, the hips, the shoulders, the chest, the upper and lower limbs.
Test results
The results of the carried out tests indicated that in hypertrophied scars and keloids treated with the compression products sweeping changes were noticed. The itch observed in 8 cases retreated after 3 weeks. The colour of fresh scars changed from bloody pale into flesh-like in 17 patients after 4 weeks. The height of the scar was reduced from average 4 mm at the beginning (measured from the healthy skin) up to 0-2 mm. The best results were observed in fresh scars, which were 4 weeks old. In the case of older scars those effects were visible after a longer period of time.
There were no allergic reactions noted. Washing by means of commonly available washing agents and an all-day-long utilisation did not affect the elasticity of the tested products. The best therapeutic results were observed on tights, lower legs and forearms. The patients had no objection to wearing the compression garments. All in all compression products Codopress® undoubtedly contribute to faster rehabilitation of patients with after-burn deformations.
The summary of test results
While wearing Codopress® products for a few months the following conclusions were made:
- the scars were getting flatter,
- the extremely red colour was gradually fading,
- no allergic reactions to the material in Codopress® products were observed,
- in the same patients comparing not pressed scar places with the ones pressed by means of Codopress® clothing there were visible differences in form of hypertrophies and hard scars in the not pressed places,
- the application of the compression clothing just after the wound was healed brought better effects than in patients who used the products after hypertrophied scars appeared. [2]

Conclusions
- The tested products Codopress® are very useful in the prophylaxis and rehabilitation of hypertrophied scars.
- Compression garments need to be tailored according to the measured body dimensions of the wearer in order to provide high efficiency.
- An early application (just after the wound is healed) of tailor-made compression products guarantees the best efficiency of the scar rehabilitation.
- Constant wear of the clothing (13 hours a day) 1 to 2 years changed only if it is worn up or the patient’s size has changed:
- prevents the development of hypertrophied scars,
- causes the reduction and, in most cases, the regression of keloids,
- improves the final aesthetic look.
- Pressotherapy enables to continue physical rehabilitation and does not constrain the patient’s activity after the burn.
- The knitted fabric used in Codopress® products causes no irritating reactions.
[separator]
Associable therapy Codopress® + Codosil™ ADHESIVE
Silicone dressings adjunctive to scar treatment by means of pressotherapy have gained in popularity in the past 10 years. Their application decreases the growth of small blood vessels in a scar, and as a result the scar gets more elastic and flatter.

Many specialists recommend the associable therapy, combining a few methods individually adjusted to a given patient. One of them is compression therapy joined with dressings meant for scar rehabiitation. The dressing used for this type of combined therapy is CodosilTM ADHESIVE.
CodosilTM ADHESIVE is a soft multi-layer product designed for the rehabilitation of hypertrophied scars and keloids. Adhesive silicone layer is in the direct contact with the scar surface. The outer side of the dressing is secured with an anti-adhesive protection layer.
- releases the itching and pain,
- does not present irritating and sensitising properties,
- is susceptible to folding,
- reveals sticky properties which makes it possible to stick to the skin’s surface repeatedly,
- is meant for multiple use,
- is easy to store and apply.
 The silicone dressing can be applied as a preventive agent when the wound is fully closed (8-10th day) or when first symptoms of a hypertrophied scar appear. Early application of the dressing increases the chance of proper scar rehabilitation.
The silicone dressing can be applied as a preventive agent when the wound is fully closed (8-10th day) or when first symptoms of a hypertrophied scar appear. Early application of the dressing increases the chance of proper scar rehabilitation.
The dressing is used only on skin that is not broken, remembering to make the dressing 1 cm bigger than the scar size. Prophylactically it should be worn 12 hours a day. In patients using the compression products Codopress® along with the silicone dressing CodosilTM ADHESIVE there were visible therapeutic effects observed: flattening, fading and softening of the scar. Moreover, the motor activity is improved and the risk of contractures is limited.
CodosilTM ADHESIVE is recommended to be used:
- in rehabilitation of hypertrophied scars and keloids,
- as prophylaxis in people with hypertrophied scar and keloid tendencies,
- in cosmetology for the rehabilitation of scars after aesthetic surgery.
Literature:
[1] Babiana Mossakowska, PhD, Professor, Presoterapia u dzieci (Pressotherapy in children).
[2] A. Nawrocki, doc., PhD, and others, Ocena kliniczna – Opracowanie technologii i ocena artykułów medycznych do zastosowania w chirurgii plastycznej (Clinical evaluation – The compilation of technologies and the evaluation of medical products to be applied in plastic surgery).
All Codopress® products are individually prepared after taking measures. To make an appointment and get more information please contact us export@tzmo.com.pl.
Michał Szymański, MD
Genesis of the disease

Stress urinary incontinence (SUI) is a civilization disease, which, given the nature of the problem, is an embarrassing and very often hidden ailment. The dysfunction associated with the described problem affects the psychophysical condition of patients dealing with this ailment. Stress urinary incontinence, as well as light and heavy incontinence forcing patients to use incontinence products such as urological liners or incontinence pull up’s pants for adults. This type of prevention does not give full comfort, discretion, and most importantly – a sense of security. However, this condition can be treated not only pharmacologically, but also surgically with the use of minimally invasive surgical techniques – through implantation of urological tapes treating this ailment permanently and giving comfort and safety.
The cause of this disease is a not properly functioning urethral closure mechanism resulting from the weakening of the sphincter muscle of the urethra or the hyperactivity of the bladder, urethra, genitourinary fistulas, dilatation of the bladder. The reasons for this dysfunction include, in case of women, inter alia multiple deliveries, damages of the urinary tract, problems with hormonal system, innate defects. For men, the causes of this condition include urethra surgeries.
The scale of the problem in the world
The incidence of urinary incontinence (UI) was estimated on the basis of 35 independent studies on a group of 230 000 people, belonging to different social groups and five ethnic groups. UI incidence in women was 27.6%, a maximum occurred in the 5th decade of life – 33%. Statistical data from departments and gynaecological and urological outpatient clinics shows that this symptom occurs in approximately 25-30% of patients over 45 years of age. It should be noted that a number of patients never report to the doctor. Every year the U.S. spends on the treatment of UI about 17.5 billion dollars (1995). It is estimated that if everyone in the U.S. who suffer from incontinence would look for help, the cost of the treatment and care would amount to $ 41 billion. Urinary incontinence hampers the normal functioning in the society and is the cause of lower self-esteem and overall well-being. The conducted studies on the population of Norwegian women showed that 46% of them identified the discomfort associated with incontinence as tedious, and 34% – as extremely annoying. The problem of urinary incontinence also has its economic aspect. It has been shown that the costs associated with having to buy the necessary medicines and personal care products exceed for about 64% the standard expenses of healthy women. It is estimated that women with stress urinary incontinence in 1998 spent for the direct aids $ 5642 USD, and the indirect measures 4208 $ U.S. These included the purchase of inserts and hygiene products, costs for professional medical help and expenses for surgical treatment. In England the budget allocated for the treatment of urinary incontinence in women is 2% of the total expenses. In the period from 2000 to 2001 there were 8000 surgical procedures because of urinary incontinence for the amount of 10.3 million pounds from the NHS funds. It has been estimated in the United States that the annual direct medical expenses of urinary incontinence are comparable and similar to those that apply to such diseases as breast cancer, osteoporosis and arthritis.
The needs of Polish market
It has been estimated that in Poland there are 20.000-30.000 procedures of urological tape implantation. However, the real need is much higher. It is assumed that approximately 30% of women suffer from this ailment, which makes about 3 million patients in Poland who should have an urological tape implanted. The percentage data concern also the global market. The tapes offered on the Polish market are available only with reusable applicators. Only a few manufacturers offer the tapes with disposable applicators made of artificial materials. The analysis of the costs associated with the purchase of tapes with applicators and comparing them to the prices of the implant can be concluded that it is more economical to purchase a product with reusable applicators. Each hospital has its own sterilisation centre and can sterilise the reusable applicator on its own, thereby reducing the cost of purchasing a disposable one. The number of sold reusable applicators represents about 1% of the amount sold tapes.
Methods of treatment
Surgical treatment is mainly used in the following cases: stress urinary incontinence, mixed form of urinary incontinence. The methods most frequently used in the surgical treatment of urinary incontinence are:
- suspension of the urethra using the tension free tape through the vagina (e.g. Tension-free Vaginal Tape (TVT), Trans Obturator Tape (TOT));
- extraperitoneal vaginal suspension (Burch colposuspension method, operations by Marshall-Marchetti-Krantz method);
- needle procedures;
- urethral injections (usually with Teflon or collagen);
- loop operations (almost entirely supplanted by TVT and TOT);
- implantation of an artificial sphincter (the highest degree of difficulty, a very rarely used treatment).
Selecting the optimal treatment method is often very difficult and depends on many factors, including: the patient’s body weight, the patient’s age, number of births and the complications associated with them, poor general health, the desire to have children, coexisting chronic diseases, doing competitive sports, experience of the operator.
The effectiveness of the chosen treatment method also depends heavily on the well performed diagnostics, which allows to determine the cause of urinary incontinence and the presence of any accompanying genital pathology.
Characteristics of TOT and TVT implantation methods
In the two treatments (TOT and TVT) the implanted product is a tape made of synthetic polymers (such as polypropylene), or of allogeneic material. Leading manufacturers of synthetic tapes are Ethicon, AMS. These tapes can also be partially resorbable e.g. the T-Sling by Polhernia company.
The set for stress urinary incontinence consisting of a urological tape and a system of applicators for TVT and TOT methods is the subject of the description of implantation methods.
In the surgical treatment of urinary incontinence in women the TVT method (Tension-free Vaginal Tape) and the TOT (Trans Obturator Tape) method is most often used – the Dallop® NM tape is intended for both of them.
TVT method
This TVT method of surgical treatment of stress urinary incontinence in women enjoys great popularity among surgeons. This procedure is performed under local anaesthesia. It takes about 20 minutes. During this procedure, the tape is introduced through the retro-pubic space, and the ends are drawn up on the abdominal fascia. This is done using special applicators designed for the specificity of the procedure. The applicators allow you to place the tape under the urethra in a safe way, providing high efficiency of the procedure, estimated at about 85% in the long-term evaluation.
The TVT method is a procedure used in the treatment of stress urinary incontinence in women performed with vaginal access, aimed at suspending the middle and posterior part of the urethra.
TOT method
The second method used more and more commonly in the surgical treatment of urinary incontinence in women is the TOT method. It is a modification of the TVT method limiting the risk associated with it. It primarily reduces the risk of puncturing the bladder or damaging the pelvic or major blood vessels. This treatment is also performed under local anaesthesia, and the duration is shorter. The big difference is the way through which the tape is implanted. For the TOT method special applicators were designed to enable taking the tape through a small space in the foramen obturatum, which reduces the risk of penetrating the bladder and allows the location of the band in a more precise and safe. This provides a method for increasing the efficiency of approximately 95%.
The method TOT uses the access through the foramen obturatum, through which the urological tape is pushed. It aims to create a kind of hammock supporting the urethra in the middle and back part.
Optimal materials /raw materials for urological tapes
Many authors of publications describing the use of various types of urological tapes, assessing the effectiveness of implanting tapes made of material of both human and animal, and synthetic origin said that the use of the tapes made of materials of human and zoonotic origin carries a high risk of complications. The most common are: erosion, infections, absorption of the tape and reduction of the initial parameters of the tapes. In addition, it is difficult to assess the effectiveness of the treatments with their use. However, the use of polypropylene tapes is free from most of these complications. Besides, the polypropylene tapes are characterised by a relatively small loss in the value of the initial parameters, what considerably affects the efficiency of procedures performed.
A randomised study on two groups of New Zealand rabbits to evaluate the response of the bladder tissue in contact with synthetic implants (the TVT tape) and zoonotic implants (SIS – Small Intestinal Submucosal – transplant of porcine origin). The third group was a control group which was subjected to a similar procedure as the other groups, with the difference that it did not have any implant. Observations were carried out for two periods of implantation – 6 and 12 weeks. As a result of these studies it was found that the wall of the bladder in contact with polypropylene showed no inflammatory reaction. Only in 3 of 12 animals the presence of fibrosis was observed. In the test group treated with porcine SIS implant in one animal a strong inflammatory response was observed, in two animals fibrosis was found. In the control group, as expected, there were no changes in the tissues of the bladder. On the basis of these observations, the authors evaluated the conclusion that both materials – both the polypropylene and the porcine SIS implant appears to be safe in contact with the tissues of the bladder. In addition, the polypropylene implant retained its morphological characteristics in the two periods of observation.
Many doctors evaluated the mechanical properties of TVT polypropylene tapes and tapes of human origin (CFL) after their implantation. These studies were carried out on rats, by selecting two observation periods 6 and 12 weeks, because in patients undergoing surgery with the use of tapes the acute tissue reaction to the presence of foreign materials usually occurs in the first three months. Two parameters of the tapes were tested: average breaking load and maximum load at break. The authors assessed that the TVT tapes retain their morphological and strength characteristics after the assessed implantation periods. However, the tapes of human origin (CFL) definitely lose their strength. Both the evaluated parameters, both after 6 and 12 weeks of observation, for the TVT tapes were almost three times higher than for the tapes of human origin (CFL). The doctors in their summary stated that such a significant decrease in the strength parameters can be the cause of low efficiency of the procedures with the application of the tissues of human origin (CFL).
Characteristics of Dallop® NM tape
Urological tape Dallop® NM meets the essential requirements of Directive 93/42/EEC for products classified as Class IIb medical devices. According to the above-mentioned Directive, Annex 9, Rule 8 “All implantable devices and invasive surgical devices for long-term use are in the Class IIb.”
Dallop® NM urological tapes are made of:
- monofilament polypropylene yarn with a thickness of 0.16 mm (185 dtex) – used to produce the main part of the tape;
- polypropylene yarn with a thickness of 0.3 mm (640 dtex) – used to make the handles allowing to fix the tape on an applicator.
Both materials are made of 100% polypropylene homopolymer and are coated with preparations in an amount of not more than 0.25%. Both yarns have a minimised elongation factor (up to 0.5% in water at 40°C ± 2°C) and the corresponding tensile strength. Drains protecting the areas where the tape and the handles are connected are made of medical PVC granulate and are used to protect the tape and the tape handles against pulling out when the tape is put through anatomical structures.
Parameters of Dallop® NM tapes:
|
No. |
Parameter |
Requirements |
|
| 1. | Breaking strength | min. 16 N | 117 N |
| 2. | Pore size | min. 75 µm | 0.38 mm2 |
| 3 | Width | 1.0 – 1.2 cm | 1.1 cm |
The Dallop® NM tapes have smooth edges and do not require additional protection, because the implant does not cause the risk of tissue damage.
The Dallop® NM tape is packaged in double medical packaging – BOM paper-film reel with a gusset suitable for ethylene oxide (EO) sterilisation. A medical device after packaging undergoes sterilisation with ethylene oxide (EO) in accordance with the requirements of EN ISO 11135-1.
The Dallop® NM tape is available in 2 sizes with a length of 60cm and 45cm, the handles are blue and made of polypropylene yarn, and the covers (drains) are made of heat-shrinkable material.
Application of the tape
The Dallop® NM tape is designed for use in the surgical treatment of female urinary incontinence by means of TVT and TOT methods. These methods are used to treat stress or a mixed form of urinary incontinence. The tape is intended to replace weakened pelvic floor muscles, which are not able to provide an appropriate angle of the urethra, leading to urinary incontinence. Creating a support under the urethra the tape restores it to its natural position.
Applicators
The provide safe implantation of the Dallop® NM tape appropriate applicators were designed: a modified TVT needle, a modified Emmet needle and curved Emmet needles (left and right). Modifications to all the applicators included adapting their ends to the fixing handles of the tapes so that you can attach the tape holder on the applicator to securely introduce the tape.
The raw material used to manufacture the applicators is stainless steel of composition appropriate for the production of medical instruments. The applicators are packed in double polythene film and a cardboard box.
The Dallop® NM tape is sold separately or in a set with applicators for a TVT and / or TOT method.



Clinical studies
Research on the Dallop® NM urological tape – produced by Tricomed S.A. and placed on the market after obtaining the CE mark and the certificate of registration was carried out in Matopat Specialist Hospital in Toruń during 01.09.2010 – 01.09.2011. Three medical obstetrics and gynaecology specialists took part in the study: Janusz Stankiewicz MD, PhD., Michał Szymanski MD, PhD, Piotr Wojtynek MD, PhD. Each of the physicians choosing patients for the clinical trial was both the operator and the person collecting clinical data from the intra- and postoperative period. The aim of this study was to evaluate the efficacy and safety of the Dallop® NM urological tape in the surgical treatment of stress urinary incontinence in women. The study included an risk assessment of complications after the implantation of the tapes and their subsequent impact on the quality of life of the patients.
Materials and methods
20 patients (women) with diagnosed with stress urinary incontinence or a mixed type of this disorder with a predominantly stress component took part in the assessment. Each patient had one Dallop® NM tape implanted; the surgical procedures were performed in the period 13.09.2010 – 08.03.2011. Characteristics of the study group: 4 patients before surgery additionally had urinary urgency. Patients’ age 35 – 74 years, (average age 52 years), BMI between 19 – 41 (average 27). All patients in the preoperative period and during the qualification for the surgery had their medical history collected, and an gynaecological examination with ultrasound performed. In all the patients the test result was positive. Before the surgery urine cultures were performed in order to exclude an urinary tract infection, the urodynamic test confirmed the presence of stress urinary incontinence.
The results took into account the data collected during the operation, after 30 minutes from the surgery, at discharge from the hospital, and within a period of one, three and six months after the surgery. All tapes were implanted with access through the foramen obturatum (TOT), this access is now preferred in most centres dealing with the surgical treatment of stress urinary incontinence as giving fewer complications, shortening the treatment time and eliminating the need for intraoperative cystoscopy compared with the vaginal access (TVT).
Description of the surgical technique: After preparing the operating field a longitudinal incision in the vagina was performed, the vaginal wall was dissected of the urethral, tunnels were created to the sides towards the obturator foramens. Through incisions in the groin folds on both sides an Emmet needle was introduced directing it through the obturator foramens to the previously prepared tunnels. The handles of the Dallop® NM tape connected to the ends of the tape were rove through the hole in the needle and the ends of the tape were led “from the inside out” by withdrawing the needle. The tape was laid without tension under the urethra, then the vaginal wall was sewed. A vaginal compression tampon was applied for a day, after the surgery the catheter was removed from the bladder, the patients urinated on their own. Eighteen operations were carried out under general anaesthesia, in two cases under regional anaesthesia – the type of anaesthesia was chosen by the anaesthesiologist in consultation with his patient.
Results of the studies
The total time of the operation: the 18 TOT operations took 10 – 30 minutes (average 19 minutes). Two operations connected with additional operating procedures (removal of the uterus, vagina wall carvings) lasted 60 minutes; the average for all the 20 patients: 23 min. Assessment of the convenience of using a tape during a surgery (0-5), (0 – cumbersome and difficult to use, 1 – very complicated application, 2 – complicated application, 3 – high degree of difficulty, 4 – small degree of difficulty, 5 – handy and easy application). In two cases the operators rated the tape at 4, in the other cases – 5 (average 4.9). After 30 minutes of surgery the pain strength according to VAS was in the range of 2 – 4, on average 2.3. The type and duration of used painkillers: all the patients were given Ketonal intravenously at a dose of 1 amp. every 8 hours, 9 patients additionally were given Morphine 1 amp. every 6 hours, 5 were given Tramal intravenously 1 amp. Noticeable discomfort on a scale 0-5 (0 – pain, I want to remove the tape, 1 – huge discomfort, 2 – big discomfort, 3 – moderate discomfort, 4 – slight discomfort; 5 – no discomfort) ranged from 4 – 5, average of 4.4. Postoperative complications such as hematoma, urinary retention, need to remove the tape, the temperature above 37.5°C, there were no signs of infection in any of the patients. Hospitalisation time took 1 – 3 days (average 1.95). At discharge from the hospital, the cough stress test result for all the patients was negative, the patients did not report any episodes of urinary incontinence. The pain strength according to VAS was 0 to 2, on average 0.6. Noticeable discomfort in the scale of 0-5 – three patients reported mild discomfort, others no discomfort (4.85 average). Postoperative complications were not observed in any of the cases. One of the patients at discharge reported occurrence of urinary urgency “de novo”. All patients reported to a control check after a month from the surgery. None of them reported any incidents of stress urinary incontinence.
Two patients with the mixed form of urinary incontinence reported the continuing urinary urgency of a similar intensity as in the preoperative period, the treatment with anticholinergics was continued. Pelvic examination: in all patients the post-operative wound healing process was correct, there was no erosion, no hematoma, no need to remove the tape, etc.. Test cough test was negative – 100% of the respondents. The pain strength according to VAS: one patient assessed as “1”, the others as “0”. Noticeable discomfort (scale 0-5) – one of the patients evaluated at “2”, one at “4”, the others at “5”, the average 4.8. 3 months after the surgery in any patient in the entire study group there was no incontinence observed. The female patient who experienced postoperative urinary urgency, treated conservatively because of the lack of improvement, severity of the symptoms, was directed to urology (cystoscopy) consultation. The cystoscopy revealed diffuse leukoplakia of the bladder, the sites of leukoplakia were dissected and coagulated (this condition was not associated with the implantation of the tape). After the cystoscopy subjective improvement and a reduction in the urinary urgency was observed. The other two patients treated with anticholinergics: in one the urinary urgency was eliminated, in the second one it was significantly decreased compared with the preoperative period. Pelvic examination: in all patients the state was correct. Cough test negative – 100% of the respondents. The pain strength according to VAS: “0”, all the patients. Noticeable discomfort: two patients “4” – slight discomfort, while the others “5” – no discomfort, the average of 4.9.
After 6 months all the patients reported for the check-ups. there was no health deterioration, there were no symptoms that may have been associated with the surgery, there was no stress incontinence. None of the patients agreed to the proposed urodynamic study before the follow-up visit considering that the treatment process is complete. Pelvic examination: in all the patients the state was correct, cough test negative. Pain strength according to VAS: the patients estimated at “0”, noticeable discomfort at “5” – 10%. The time to return to full active life after the operation ranged from 1 – 8 weeks, on average 2.9 weeks. The patients assessed that their condition improved after surgery.
Summary of the studies
In the study group of 20 patients with stress or mixed type of urinary incontinence during the 6 months from the implantation of the Dallop® NM urological tape by means of the TOT method, there were no significant intra – and postoperative complications associated with the implant. The tape was evaluated by three operators involved in the study as a handy, convenient to use and safe. The duration of the implantationof the Dallop® NM tape with access through the foramen obturatum access was short (on average about 20 min.). The pain and discomfort associated with the surgery in the patients was short, low-graded. Most of the patients returned to active life after the operation within 2 – 3 weeks, within six months all patients found their health as better compared with the preoperative period. Efficacy in the treatment of stress urinary incontinence in the study group was defined as 100% in terms of subjective (interviews collected from the patients) and objective (pelvic examination with a cough test) opinions.
Conclusions
- Based on the results of the six-month observation of the operated group of twenty women, the Dallop® NM urological tape can be considered as an effective, convenient for doctors and patients, and safe method for the treatment of stress urinary incontinence in women.
- In the examined group all the patients achieved good results of the surgical treatment and there were no complications associated with the surgical procedures and the implanted tape.
Elżbieta Szwałkiewicz
National Consultant in Nursing Chronically Ill and Disabled People
Even the most modern, well-matched to the wound type dressing will not facilitate the wound healing process if additional conditions conductive to further body regeneration will not be met.

These are:
- proper body hygiene,
- skin protect against irritating effects of urine,
- suitable bed, mattress, bed linen and underwear,
- elimination of pressure on the part of the body affected by a bedsore,
- safe movement and positioning of the body,
- adequate nutrition and hydration.
Modern technical solutions and technologies allow for the safe performance of hygienic activities, even in those patients with very sensitive skin and completely immobilised, without the risk and effort associated with their movement. On the market there is a wide range of skin care, hygiene facilitating devices available. When dealing with dry skin (frequently washed with soap), weakened, macerated, constantly subjected to the action of irritants, it is necessary to check the condition of the skin daily looking for signs of an allergic reaction. Appropriate preparations for cleansing and skin care of the sick are the ones that can be applied to sensitive and irritated skin, and have moisturising, greasing and elasticising properties. They should alleviate symptoms of inflammation, grease and protect the skin against irritants such as urine. For irritated and itchy skin soap should not be used only mild cleaning agents (lotions, foams). It is advisable to use cosmetics with as little allergic reactions as possible. The used cleaning and care products should be manufactured in sets by the same company as this will prevent the use of products of different chemical components coming into harmful interactions for the organism. Just wash the wound area, and always check the condition of the wound dressing and protection of the wound against pollution and getting wet during hygiene procedures.
Unpleasant for the patient and his/her environment urine odour can be eliminated by proper selection of absorbent materials and their appropriately frequent change – about four times a day. While changing be sure to cleanse the abdomen, genitalia, groin and buttocks.
A patient who cannot change the position from lying to sitting can be washed traditionally in bed, but can be also bathed in a special movable bathtub. The bathtub is taken into the patient’s room, one side wall is removed and is set along the bed. Then, using a cloth or a special sliding mat to move the patient (previously undressed and covered) into the tub. If the patient is on a drip, monitor, respirator, etc., the bath is carried out in the room next to the bed. This is possible when to the sink tap (located in the room) a shower hose of suitable length with a shower head is attached. Similarly, the drain hose must be of appropriate length to reach to a special outlet installed under the sink. If the patient is able to leave the room, he/she is taken on the bathtub to the bathroom with a shower post. The drain hose is introduced into the floor drain. Bathing in the supine position can also be done in a bathtub with an adjustable height. A person who cannot move, is moved (undressed and covered) by sliding onto a special man lift – a kind of trolley-stretcher. Following the transfer of the patient to the bathroom, the lift is placed on the bath, which rises (electric mechanism operated by means of a remote control) to the height appropriate for the carer, so that he/she does not to have to bend down. Then, the lift with the patient is lowered to the bottom of the tub. Most of the mentioned bathtubs has also an incorporated hydro massage device. The lift has the ability to raise the head rest so that the patient can be washed in a sitting or reclining position. In a set with the bathtub there are also available chair lifts that help people with paraplegia or the disabled to get to the bathtub and leave it. These people can also wash themselves in the shower using the lift or a sanitary chair. All institutions where there are patients with locomotor disabilities should have integrated systems for personal hygiene i.e. movable equipment integrated with cleaning equipment.
People unable to walk e.g. with paraplegia can use the toilet alone but there must be conditions created enabling the move from the wheelchair onto the toilet. The height of the toilet and the wheelchair should be similar. The side walls of the chair and security handles at the toilet should be tippable. Within easy reach of a person using the toilet there should be a shower head to wash and toilet paper to dry the skin. The ability to wash oneself with running water is highly important, because it is very difficult to clean the genital and anal area with toilet paper. In elderly people the skin is wrinkled and therefore its thorough cleaning off stool remnants is not possible by means of dry toilet paper, and repeatedly rubbing the sensitive and dry skin often leads to its damage. In the toilet there should be enough space for a disabled person to drive a wheelchair, park along the toilet, and after picking up the side part of the chair and the toilet handle, move onto the toilet. All people, regardless of their health and fitness, should be able to use the toilet. It should be kept in mind that when lifting and moving the patient strong point pressure on the body ought to be avoided and the sliding method to rotate the body ought to be applied. The need to clean and protect the skin is particularly important for people with disabilities who face the problem of urinary incontinence.

Please note that urine in contact with the skin is an external irritant, causing inflammation. The inflamed skin is red, irritated and painful. There appears also often swelling, itching and flaking of the skin. Patients trying to reduce the annoying itch scratch themselves, and ultimately break the continuity of the skin, leading to the formation of wounds. These scratches are the site of bacterial infection and the development of complex infected bedsores.
The desired effect can be achieved using hygienic disposable absorbent materials, sets for urine collection, specialist personal hygiene and cosmetic and protective preparations. Their offers is very rich in the market.
Diapers, anatomically shaped diapers or urine pads should be chosen according to their absorbent ability, the content of a urine binder, the type of protection against the leakage from the diaper, the ability to reduce unpleasant odours and the possibility to closely adjust to the body. It is also important that the absorbent body is covered with special nonwoven, which also separates the urine absorbed from the skin.
Urinary incontinence leads to constant moisture and maceration of the skin, which promotes its inflammation, damaging, resulting in the formation of bedsores. Therefore, it is necessary to systematically check the condition of the skin in areas exposed to moisture and the state of dressings, and maximally shorten the time of skin contact with urine.
Therefore, the selection of an absorbent product should be determined by the degree of urinary incontinence, the patient’s level of consciousness, time of the day and level of activity. People with pressure ulcers or very sensitive dry skin prone to irritation, should use the so-called breathable diapers. They differ from other diapers for instead of the protective film they have to a special air-permeable laminate.
While nurturing a bedridden person with urinary incontinence (UI) it necessary to use hygienic underpads to maintain the cleanliness of linen or to secure the chair. Do not use rubber underpads but pads made of cellulose with one side coated with special film protecting the chair or the bed against wetness. Here also breathable absorbent products should be applied. People with bedsores should avoid overheating in warm clothes and airless or overly heated rooms, and above all, they should avoid long-term pressure on the damaged skin and skin friction over the ground. This effect can be achieved by using a special sliding and equipment for sliding repositioning, pressure relief mattresses and pillows, frequent change of body position, the application of proper rules for lifting and moving the patient.
Significant reduction or elimination of pressure on the skin can be achieved by equipping the bed with an anti-bedsore mattress:
- alternating pressure (so-called dynamic) anti-bedsore mattress where a motor pumps air into individual chambers of the mattress, filling them only some of them which allows to temporarily relieve another part of the body. Using the mattress does not cancel the obligation to adequately frequent change body position.
- constant pressure anti-bedsore mattress, pumped using a hand pump, enabling to achieve appropriate pressure and reduce the pressure on the body surface. It is also important that it is made of a material with a unique antibacterial formula inhibiting the growth of bacteria and odour inhibitor. Using this mattress has a preventive effect and accelerates healing of existing wounds. This mattress is particularly useful in patients who dislike the sound of the pump motor in the dynamic mattress.
The time of healing a bedsore or any other chronic wound depends on the general state of health and on good nutrition with adequate supply of protein, calories and fluids.

The operating room, a special place in the operating suite and throughout the hospital, it must comply with the relevant conditions providing safety for patient and staff – to carry out the operation. In the operating room there should be maintained increased health regime, so that it does not become a place where a patient can get infected. Accordingly, the operating room staff requires to maintain specific discipline, show high expertise and relevant skills.
Contemporary built operating suites have air-conditioned operating rooms, thus eliminating the need to install radiators in such places (habitat of dust and pathogenic microflora). The lack of windows also limits the access of air pollutants (mainly bacteria and fungi).
All the operating conditions should be created to safely perform surgical procedures, in accordance with the principles of asepsis. The layout of rooms forming the operating suite should be divided into a dirty, clean, and sterile area and force a one-way movement of staff, patients and sterile material. To ensure the safety of the performed procedure, attention should be paid to all the particular stages, starting with the preparation of material required for the procedure.
Taking an example of a knee arthroscopy procedure we want to show how to properly protect a patient using the components of the set.
All the used elements are the components of the OP-set.
BEGINNING OF THE PROCEDURE




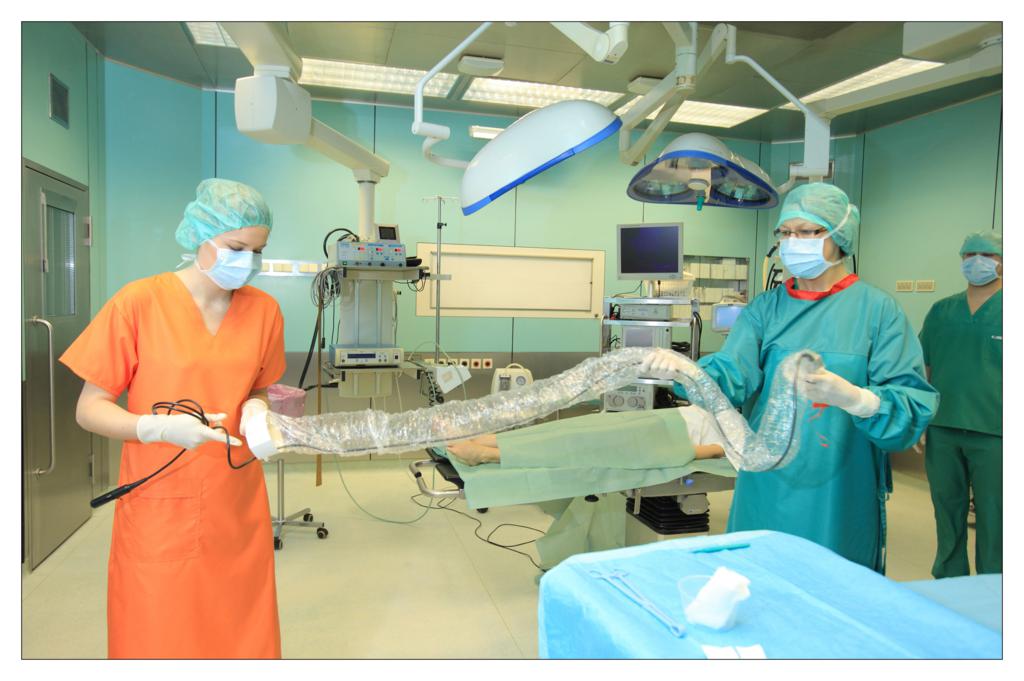




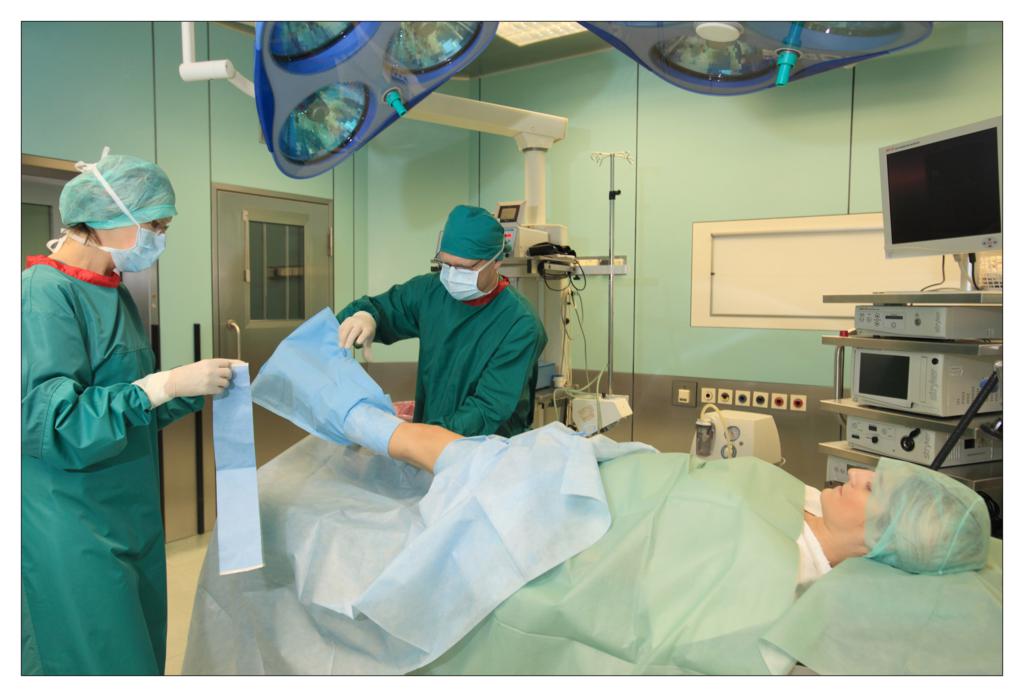




FINISHING THE PROCEDURE


Beata Ochocka
National Consultant for Epidemiological Nursing
In history there are no control groups. Nobody knows what would happen if things went a bit differently.
Cormac McCarthy
Crazy evolution of the virus – “All replicate on the road of dissolution and the subsequent reconstruction” Roland Wolkowicz, a molecular virologist from San Diego State University. “Are we endangered by hunger and epidemics?” – an interview with Joel Cohen, an eminent biologist, a specialist in research on populations. These are just two examples of media reports in recent months. Humanity of the turn of the centuries has many dilemmas and problems, economical, political, these concerning access to clean water and food. These concerns are for nothing since the fundamental problem is, and will be, to protect human health. In the context of the hospital-acquired infections, causes of public health problems include unseen growth of multi-refractory strains, a decreasing number of new effective antibiotics, the lack of vaccines, complex systems of bacteria and virus resistance (MDR XMDR – resistance of bacteria to some or all treatment groups). As the dangerous phenomena of the last decade we must also include winning bacterial biofilms with system “quorum sensing”- somewhat contemporary Enigma cipher. Former “hospital hyenas” return, including Pseudomonas aeruginosa, Acinetobacter baumannii. The result is alarmingly increasing mortality and the incidence of hospital-acquired infections among patients in almost all countries. Claims for infections have become a commonplace element in the functioning of Polish health care and routine activities of law firms specializing in medical cases. The situation in the field of infectious diseases is similarly unfavourable. The old, so-called recurrent contagious diseases (“re-emerging infectious diseases”) returned. An example of anxiety of CDC is pertussis causing, in a global scale, 40 million cases of illnesses and 350,000 deaths annually. At the end of last year, because of the Polio situation, special alerts were declared; the warnings were also made in our country. In 7 countries, including Egypt- so willingly visited by Polish people, there began a massive campaign of additional vaccinations which will target 22 million children under the age of 5. The world is still endangered by “the dirty dozen” of Ebola, cholera, plague, tuberculosis, Lyme disease, and avian influenza.
As the consequence of the development of medicine, including huge progress in the use of surgical and invasive procedures, there appeared hospital infections, HAI.
In these dangerous times of expansion of virulent pathogenic microorganisms, we must ensure hospitalized people with current and highly effective protection against infection, including people undergoing surgery. The history of surgery dates back to the Paleolithic era and runs through the first “operational guidelines of the operating room,” Hippocrates, Galen work, hospitals in shelters and hospices, to achievements of Morton, Bergman, and Mikulicz. Contemporary operating blocks are the most expensive parts of hospitals using sequences of zones of increasing cleanness level. However, it is worth to invest in these areas, in order to obtain the highest possible standards of treatment. In Poland, there have already been applied another ordinance of the Minister concerning the professional and sanitary requirements and developing and implementing of block equipment; to some extent these restrictive regulations impose overcompensating arrears generated in many hospitals throughout the decades of the last century. Prevention of surgical site infections does not apply to a single unit of the hospital: operating block or department. In the case of, both, the department and the operating block, but also in diagnostic laboratories and all the other auxiliary places for those units- there is no room for discretion/arbitrariness in the behaviour of the staff. Hospital acquired infections (HAI) belong to one of the most common clinical form of hospital infections. They are the cause of increased morbidity and mortality of patients, the extended duration of hospitalization, increased treatment costs, damages, but most of all, unfavourable social impacts, such as job loss, including having a great significance consequences of personal distress and suffering of patients and their families.
The history of surgery dates back to the Paleolithic era and runs through the first “operational guidelines of the operating room,” Hippocrates, Galen work, hospitals in shelters and hospices, to achievements of Morton, Bergman, and Mikulicz. Contemporary operating blocks are the most expensive parts of hospitals using sequences of zones of increasing cleanness level. However, it is worth to invest in these areas, in order to obtain the highest possible standards of treatment. In Poland, there have already been applied another ordinance of the Minister concerning the professional and sanitary requirements and developing and implementing of block equipment; to some extent these restrictive regulations impose overcompensating arrears generated in many hospitals throughout the decades of the last century. Prevention of surgical site infections does not apply to a single unit of the hospital: operating block or department. In the case of, both, the department and the operating block, but also in diagnostic laboratories and all the other auxiliary places for those units- there is no room for discretion/arbitrariness in the behaviour of the staff. Hospital acquired infections (HAI) belong to one of the most common clinical form of hospital infections. They are the cause of increased morbidity and mortality of patients, the extended duration of hospitalization, increased treatment costs, damages, but most of all, unfavourable social impacts, such as job loss, including having a great significance consequences of personal distress and suffering of patients and their families.
The occurrence of infectious complications related to the surgery on which we have influence, can be effectively constrained and reduced to a safe level.
Among others, through the proper hygiene of the treatment environment, hygiene of the patient being treated, following the anti-epidemic procedures in surgical departments and treatment rooms, personal hygiene and the use of appropriate peri-operative preventive measures and all other activities in the sphere of protection of surgical site against infection. During the budgeting period it is worth to spend a larger part of the hospital funds on the hygiene and prevention of hospital-acquired infections. Money spend in this way will bring profit.
The latest data on hospital infections comes from a European spot survey made on the EU member countries and from Croatia, additionally conducted in 2012. It is published by the report of European Centre for Disease Prevention and Control, ECDC. The study assessed the overall prevalence rate of infections associated with healthcare in Europe at 6%. Poland received slightly higher percentage – 6.4%. The base of the entire study were information taken from 947 European hospitals. Our country illustrated the data from 36 hospitals that meet the criteria of the protocol; most numerous in the study were provincial and specialist hospitals – 27.8%, clinical and highly specialized – 19.4%. In Europe dominated clinical hospitals – 31.8%. The number of patients in the study was over 231,000, including Polish patients – more than 8,000. In my opinion, it is an interesting fact that more European than Polish patients were taking antibiotics – 35% vs. 31.9%. European treatment departments received the level of infections above the overall average for SSI – 6.9%. Polish treatment departments received a result below 6% of general and treatment morbidity – 5.6%. For the most common clinical form of hospital infections, hospital-acquired infections ranked in second place after pneumonia (Europe 19.6% vs. Poland 20.2%). The difference between these two figures was low- 0.2% .The bigger differences between European and Polish data concern infections in paediatric departments.
Reports from Polish research centres in recent years illustrate the importance of the HAI problem in patients undergoing surgery. The two-year study of Giedrys – Kalemba on a population of nearly 300 kidney recipients in Western Pomerania proved that it is a very important clinical problem in transplantology. In this study, surgical site infection, which was diagnosed in patients after kidney transplantation, was located in a third place with a rate of 7.6% in researched clinical centre and 12.9% in the hospital of the provincial rank. It should be noted that an increasing number of branches engaged in organ and tissue transplantation environment devoid the natural micro flora.
Document of the European Centre for Disease Prevention and Control, ECDC, describes in detail definitions of surgical site infection (HAI, SSI). They were developed by an international group of experts in 2009, in order to unify criteria for diagnosis of infections as part of their monitoring, in all European Union and cooperating countries. They are mainly based on IPSE / HELICS definitions used so far, and supplemented by definitions of the US CDC infection of the newborn. In the range of SSI definition, there were highlighted and described in detail: superficial infection at the incision site, deep incision site infection and infection of the organ / site. Recognition of these cases is based on the criterion of clinical symptoms, isolation of microorganism and the appearance of the symptoms.
It is confirmed that the risk of SSI prevalence is correlated with the risk of the procedure and depends on the patient’s general condition. Illustrating the likelihood of SSI for the same treatment in a patient with low risk – in a patient at high risk, it may even be several times higher. The literature states that the incidence rate of infections after surgery in the clean site is approximately 2%, in the dirty, infected zone it may reach above 30%.
Infection control is the basic standard for the proper care of hospitalized, operated patients.
The program of infection control at the surgical site should include the study, control and analysis many of the issues carried out in cooperation with numerous departments of the hospital: the technical, functional and sanitisation conditions, organization of work, shortening the length of stay of the patient in the hospital before surgery, the implementation of a set of basic steps to prepare a patient for surgery, system of supervising and monitoring adherence of hand hygiene, asepsis and antisepsis, proper planning of procedures, prophylactic use of antibiotics, targeted antibiotic / antibiotic therapy, level of insulation, active monitoring of infections and alarming factors, continuous training courses, hygiene of ward, dealing with underwear and medical waste, profession control, immunization and health surveillance of the personnel correspondingly with the requirements of use of medicinal products and medical devices.
To the factors enhancing the risk of hospital infections of surgical site, mentioned at the beginning of the article, there should also be included decontamination challenges: cleaning, disinfection and sterilisation of specialized equipment in surgical wards. Procedures for medical, nursing and assistance proceedings undergo very dynamic changes. On one hand, changes generate progress, provide access to effective and rapid treatments, on the other hand, new technologies and materials for treatment, such as: implants, wound dressings, drainage system, skin disinfection, surgical techniques, improperly applied and decontaminated medical devices may be source for undesirable events.
In every surgical ward, each instrumentalisation favours infection, and the action performed aseptically reduces the risk several times. Another important cause of infections in patients undergoing treatment is the repeated interruption of natural skin-mucosal barrier. It is very dangerous and conduces a high risk of haematogenous infections. Vascular lines, nutrition, parenteral nutrition, tests … the gates of dozens of potential infections. How much knowledge about infections and concern is needed of people working in surgical wards! But treatment and care are not only on an outpatient basis, but also elements of psychology, “healing with words”. One of the basic, reliable principles of infection prevention was, is and will remain, hand hygiene. This is the easiest method of preventing surgical site infections for their most common cause is the transmission of bacteria between patients on the hands of staff. Hand hygiene must be understood in a complementary way, which means applying to all but the staff, patients and visitors, including a hospital chaplain, lab assistant, radiologist, nutritionist, trainees and students. For over a year, in Poland, there is a WHO campaign, promoted by many individuals and institutions, which is aimed at raising the discipline of obeying cleanness of hands in medical facilities “Clean care is safer care”. Hospitals are counting the amount of consumed resources, held conferences, actions and appeals. These are needed, but I hopefully anticipate time (organically, working in the field of education at basis) when this cheap and simple habit will be instilled in our professional credo as a natural reflex, without which we will not perform specific tasks at patient and in the treatment environment both closer and further.
The presence of various resistant strains of bacteria in the aetiology of surgical site infections requires sound knowledge and proper control by the hospital Infection Control Team. However, it should be required from the entire therapeutic team, led by department manager sensitive to the issue of hospital infections, physician in charge of the patient, to recognize the infection rapidly, early implemented therapy based on antibiogram and widely understood cooperation with epidemiology specialists. There are no such hospitals in the world where their good hospital flagship will have a zero rate of hospital-acquired infections. This situation is not acceptable! This is a bad flagship. Hospital infections have been, are and will be an inevitable concomitant component of treatment, especially hospitalization, treatments. But they must be minimized, controlled. Polish epidemiological nursing, not only in my opinion, has achieved so much success and has contributed most effectively to change the image of the fight against infections in the last fifteen years, co-creates modern model of infection control. There’s a place for everyone. These successes bring more joy, because in no fully satisfactory economics of hospitals, the introduction of verified in other countries facilities and solutions – is much more difficult. In my opinion, the current treatment procedures include those solutions and, what is most important, these procedures work in practice. All records are now proceeding algorithm for clinicians, but in the context of infections, proceeding in accordance with the procedure confirms the concern for patient safety. One of the world’s most widespread assessment of the patient state before surgery is the scale of ASA. It punctuates health depending on the basic disease and the clinical condition; studies show that the results of measurements conducted by its use correlate with the incidence of SSI. The more risk factors, the higher risk of complications and death of the patient. The image of contemporary infectiology causes that the surgeon has contact with microbiological challenges beside the therapy and diagnostics.
Infectious complications significantly delay recovery of the patient after the surgery performed. Microbes colonizing the skin and mucous membranes of the patient are a serious source of infection.
Nearly half of infections after surgery in the clear area is the result of contamination of the patient’s own flora. The risk of SSI increases due to the presence in the body of the patient dangerous inflammations and trans-located by haematogenous way of bacteria to the wound. A significant problem in surgical patients is carriage of Staphylococcus aureus strains, an emergency situation is the finding in a patient MRSA resistant strain. Determined with the presence of hospital epidemiologists, groups of patients (recipients of organs, patients with large deficits of immunity, long-term antibiotic therapy, being under the long-term care and ICU, others with a high index of risk of infection) should be monitored and diagnostic material should be taken at the time of admission to the ward or before the scheduled admission in order to carry out decolonization. These include: eradication of nasal part, decontamination of the body, the use of isolation as a primary means of protection against cross infections and dangerous for surgical wards epidemic outbreaks, which can quickly hinder or prevent the normal rhythm of ward’s work. Recent studies have shown that the benefits of simple and inexpensive procedures of decolonization is more effective than previously thought in comparison to the administration of drugs, including vancomycin. Another warning should be added. At the end of last year, very disturbing information started to reach the Polish epidemiologists about the significantly high percentage of MRSA infections in Polish hospitals in recent studies. So, another “hospital hyena” shows its merciless face, and MRSA remains one of the most important factors that cause surgical site infections. Considering the SSI subject a significant problem for surgery, concerning infections caused by Clostridium difficile, should be signalised, which main reason is, among others, antibiotic therapy. Each diarrhoea must be diagnosed. Part of the patients treated in surgical wards meet the criteria for the development of this infection; it is important for the personnel’s conduct to be marked by strict obeying of the regime against the risk of environmental contamination of spores. CDI accompanying patient after surgery significantly impairs the healing process. In 28% of patients with primary infection with Clostridium difficile, relapsing can be observed.
Reducing the risk of developing SSI
In this part of article about so invariably important problem for operated patients, their families and for us- physicians, fulfilling and supporting from different parts the safe process of a patient’s stay in hospital, there is an opportunity to remind few aspects of the recommendations of reducing the risk of developing SSI, which I gave in my opinion as a national consultant in 2010:
- in the day preceding the surgery and the day of surgery, prepare the patient’s skin by bathing the whole body with the use of professional antiseptics,
- for patients with confirmed bacterial colonization or infection caused by methicillin-resistant Staphylococcus aureus, skin decontamination should be carried with means of proven efficacy biocide,
- in the day of surgery, under general anaesthesia, on a patient should be carried out disinfection of the oral cavity with the use of a professional antiseptic to reduce bacterial bio film,
- if the hair cannot be left around the cut site, preoperative hair removal should be performed in the shortest possible time from the beginning of the surgery with the use of cutting or depilatory methods (blade must be used once),
- for surgical procedures, clothing and barrier materials should be used,
- principles of perioperative antibiotic prophylaxis should be strictly abided,
- the number of people in the operating room should be limited,
- in the ward and the operating wing aseptic and antiseptic rules should be absolutely abided,
- medical devices should be used in accordance with rules and the rules of sterility of products and how to use them should also be abided
Introduction to surgery the techniques for minimally invasive surgery (MIS), robotisation, peri-operative medicine concepts, the idea of an integrated operating wings, allows surgeons to use their skills with intensified strength and personnel for more comfortable work. Will it be enough to deprive the patient of adverse consequences, complications, and above all, to eliminate or reduce SSI? In my opinion – no. Knowledge, diligence and conscientiousness of the staff are the basis for effective prevention of hospital infections. In infection control, abidance of recommendations is a key to success, into which also patient and his family should be involved. In the surgical wards invaluable are the procedures for hand hygiene, catheter related infection, peri-operative prevention, proceedings towards a patient with KPC, MRSA and Clostridium difficile. Polish Association of Epidemiology Nurses in its scientific notebooks and quarterly “Nurse Epidemiology” refers to many aspects of protection against hospital infections concerning the medical staff, these positions are available and can be a very good and reliable complement to treatment clinical knowledge.
At the end…
What complicates the risk situation? It might be worth to look at this meaningful list, to which once again from many years the history of infections added another verses:
- overpopulation and easier migration between countries,
- aging of the population, immunological disorders,
- gathering of people exposed (the flow of patients in hospitals),
- resistant bacterial pathogens,
- overcoming barriers between species,
- lack of medical personnel.
- drug abuse and antimicrobials (selection of resistant strains)
- invasiveness of medical procedures.
- substitution of animals, food, plants,
Waiting for “miracle drugs” such as what once was penicillin and subsequently occurring after them therapeutics, we shall accept with humility the principle that at this stage of treatment we favour the principle of “cleanness reasserts us health, and our patients….” and necessarily follow the instructions and medical procedures preventing infections!
Literature:
- Deptuła A. Pierwsze ogólnopolskie badanie występowania zakażeń związanych z opieką Zdrowotną i stosowania antybiotyków( EU-PPS HAI&AU) – różnice pomiędzy Polską a Europą, Kraków: XX Zjazd PTZS; 2013
- Giedrys – Kalemba S. Zakażenia u pacjentów po przeszczepieniu nerki – doświadczenia własne Kraków: XX Zjazd PTZS; 2013
- Izydorczyk E. Praca pielęgniarki na bloku operacyjnym, Magazyn Pielęgniarki Operacyjnej 8/2013
- Bober – Gheek B, Fleischer M Podstawy Pielęgniarstwa Epidemiologicznego, Warszawa: CKPPIP; 2002
- Definicje zakażeń związanych z opieką zdrowotną (HAI), ECDC, NPOA, www. antybiotyki. edu.pl
‘Wound’ definition
A wound is damage to the skin and sometimes to deeper underlying tissue and even organs as a result of mechanical, thermal or chemical injury. The wounds caused by mechanical injury include: abrasions, cuts, cracks, stab wounds, bite and surgical wounds. The wounds caused by thermal or chemical injury include: all kinds of thermal, chemical, electrical or radiation burns. There are certain types of wounds – chronic (non-healing) wounds, which are caused by other processes – disease processes. Chronic wounds include: pressure ulcers (trophic ulcers), venous ulcers, neuropathic ulcers and ulcers caused by infections and as a result of radiotherapy or neoplastic processes.
Types of wound healing
1. Slowly healing wounds – healing by granulation
- significant loss of tissue
- the wound cannot be closed by using physical methods
- long healing time
- the treatment is based on the processes of tissue reconstruction – the defect fills in with granulation tissue, on which epidermis appears and forms a scar
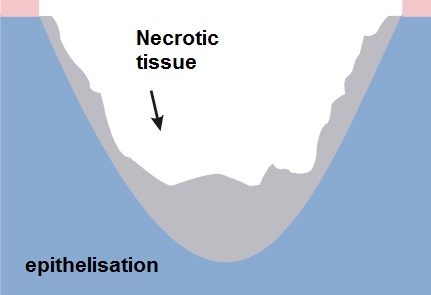
2. Acute wounds – temporary healing by first intention
- surgical or fresh traumatic wounds
- minimum loss of tissue
- edges are joined by seams or using a plaster
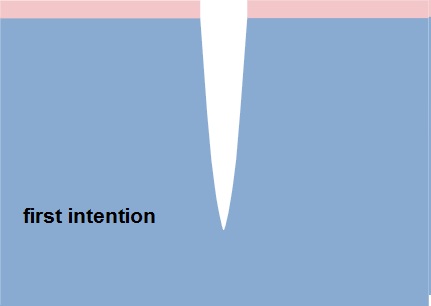
Healing phases
There is no one universal dressing that can be used in each case.
Dressings have different functions: cleansing, absorbent and protective, they often complement each other and none of them alone can meet all the needs of the wound passing through the healing stages:
- inflammation phase (exudate)
- granulation and epithelisation phase (growth)
- maturation phase (reconstruction)
Inflammation phase (exudate)
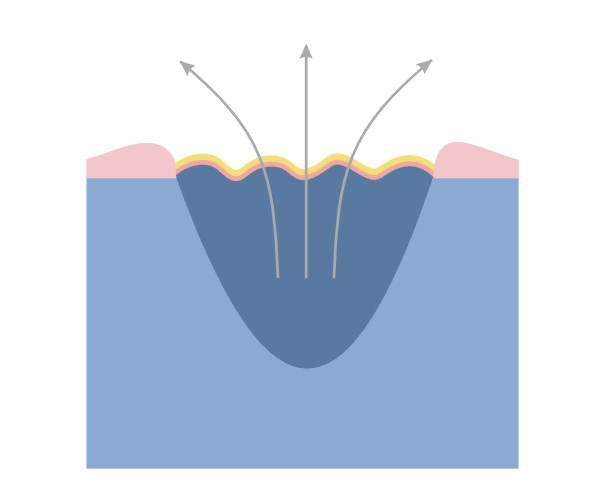
This phase is the body’s response to an injury. Due to circulatory disorders, enlargement and increased permeability of capillaries oedema occurs, accompanied by exudate.
Functions of the dressing in the inflammation phase:
- stemming the bleeding
- facilitating natural debridement
- absorbing excess exudate
- preventing re-infection
Granulation and epithelising phase (growth)
Granulation – the change from the inflammatory phase into the proliferative phase, which is controlled by macrophages and other cells. Macrophages stimulate fibroblast growth.
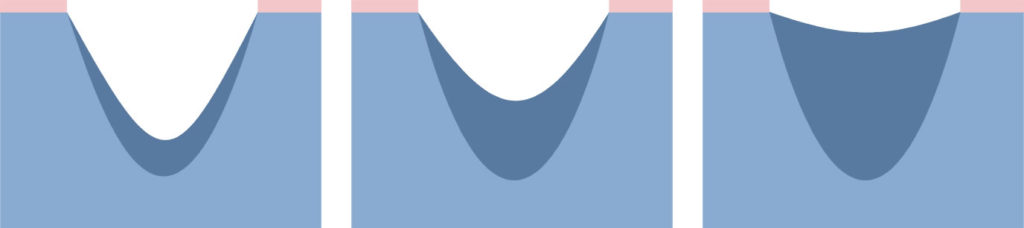
Fibroblasts fill the space that is left after the lost tissue with granulation tissue.
Narrowing of the wound – many fibroblasts is transformed into myofibroblasts. The network of connected myofibroblasts pulls the edges of the wound together (0.6-0.7 mm/day).
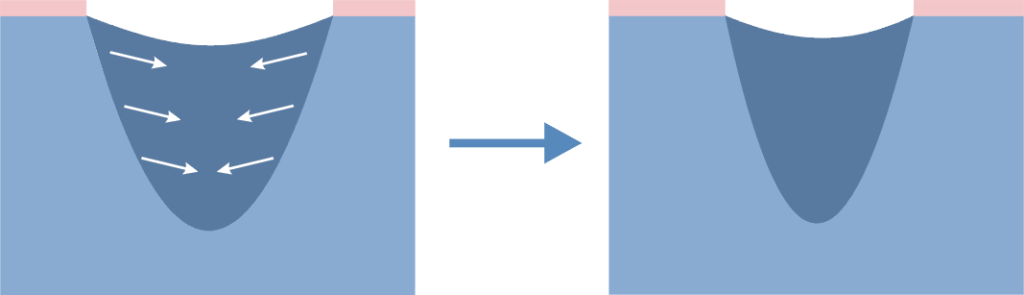
Narrowing of the wound makes the scar smaller than the original wound.
Epithelisation – new epidermis, which is needed for the complete closure of the wound. Epidermal cells migrating from the edges of the wound cover the granulation tissue and create new skin.
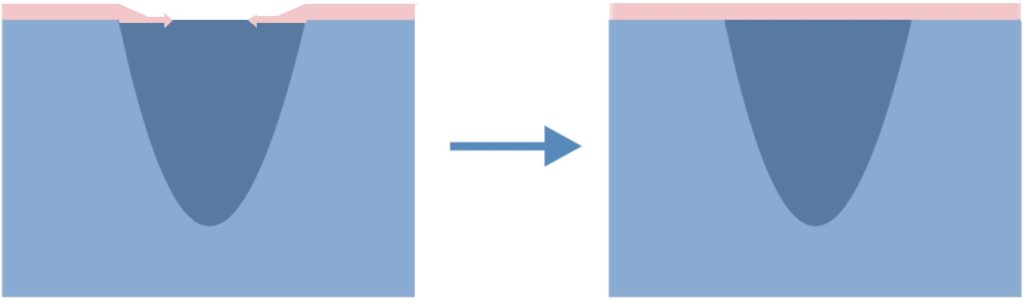
Functions of the dressing in the growth phase:
Granulation
- maintaining moist environment
- absorbing excess exudate
- protecting against mechanical injury
- preventing re-infection
Epithelisation
- maintain a moist environment
- protecting delicate epidermis during dressing changes
Maturation phase
Maturation – slow reorganisation of microscopic structure of scar tissue; the remodelling results in improving the strength of the scar, its reduction and smoothing.
This stage can last for months or even years.
In the treatment of abnormal scarring are the following items are used:
- topical silicone dressings
- compression bandages or special compression garments
- surgery, corticosteroid therapy, laser and cryosurgery
Functions of the dressing in the maturation phase:
- smoothing the scar
- whitening the scar
- reducing the scar
What is wound exudate?
Wound exudate is a particular fluid called in the past “nature balm” appears in the first stage of wound healing, immediately after an injury.
The exudate contains a variety of ingredients including nutrients for actively metabolising cells:
- very few red blood cells
- up to 6 times more white blood cells than in the blood
- less glucose, but the same amount of minerals as the blood
- proteins – among which there are enzymes important for the wound healing processes; the released enzymes cleanse the wound and remove damaged tissues
In a normally healing wound the amount of exudate decreases with time. In a wound, in which the healing process is disturbed, the amount of exudate is not reduced in time and its management can be a big challenge for dressings.
NOTE: to maintain the best possible conditions for wound healing the optimal amount of wound exudate is needed, namely a so-called moist wound healing environment.
Too much exudate and its absence can slow down the healing process. Therefore, it is important to choose an appropriate dressing to the amount of wound exudate. In wounds dry without exudate the dressing should moisten, and in wounds with too much exudate preferably the dressing should absorb its excess.
NOTE: The change in colour, odour and exudate density may indicate a change in the wound or the appearance of inflammation / infection – it is a signal that the wound should be examined and assessed by a specialist.
Dressing type vs. indication for its use in wounds with various exudate amount
| Dressing type | Level of exudate | ||||
| none | low | medium | high | medium/high | |
| challenge for the dressing | hydrate the wound | maintain a moist environment | absorb the excess of exudate | absorb the excess of exudate | drainage of excess exudate to the secondary dressing |
| hydrogel | √ | √ | |||
| polyurethane film | √ | ||||
| hydrocolloid | √ | √ | |||
| polyurethane foam | √ | √ | |||
| alginate | √ | √ | |||
| resorbable | √ | ||||
Wound treatment models
The traditional wound healing model
Through the centuries chronic wounds were treated using a variety of materials that were to dry the wound.
The traditional wound treatment system based on the use of absorbent dressings made of gauze which:
- ensured the absorption of excess exudate
BUT
- failed to protect the wound against drying out and cooling down, which slowed down the rate of healing
- did not constitute adequate protection against external factors, which could lead to frequent wound infections
- adhered to the wound, which damaged the new tissue and caused pain to the patient during dressing changes
- with limited absorptive capacity compelled to frequent dressing change
Dry wound healing is still the most desirable but for acute wounds healing by first intention.
The modern wound healing model
Since the publication of research by George Winter, it became clear that wounds heal much more quickly if the healing process is carried out in humid conditions in which the optimal amount of exudate is maintained on the surface of the wound. In view of the conditions under which the treatment process takes place, the concept was called A MOIST WOUND HEALING.
According to this concept, the treatment deals with closing the wound with a special dressing which:
- maintains the required level of moisture on the wound surface to create an optimal healing environment
- initiates autolytic cleansing, which leads to faster debridement and to start the healing process
- thermally isolates the wound which keeps the temperature at a constant level and accelerates the healing process
- provides long-term absorption of excess exudate, reducing the number of dressing changes
- does not adhere to the wound thanks to which dressing change is safe for young tissues and painless for the patient
- is water-resistant and protects the wound against external environment, which minimises the risk of infection
Features of a perfect dressing
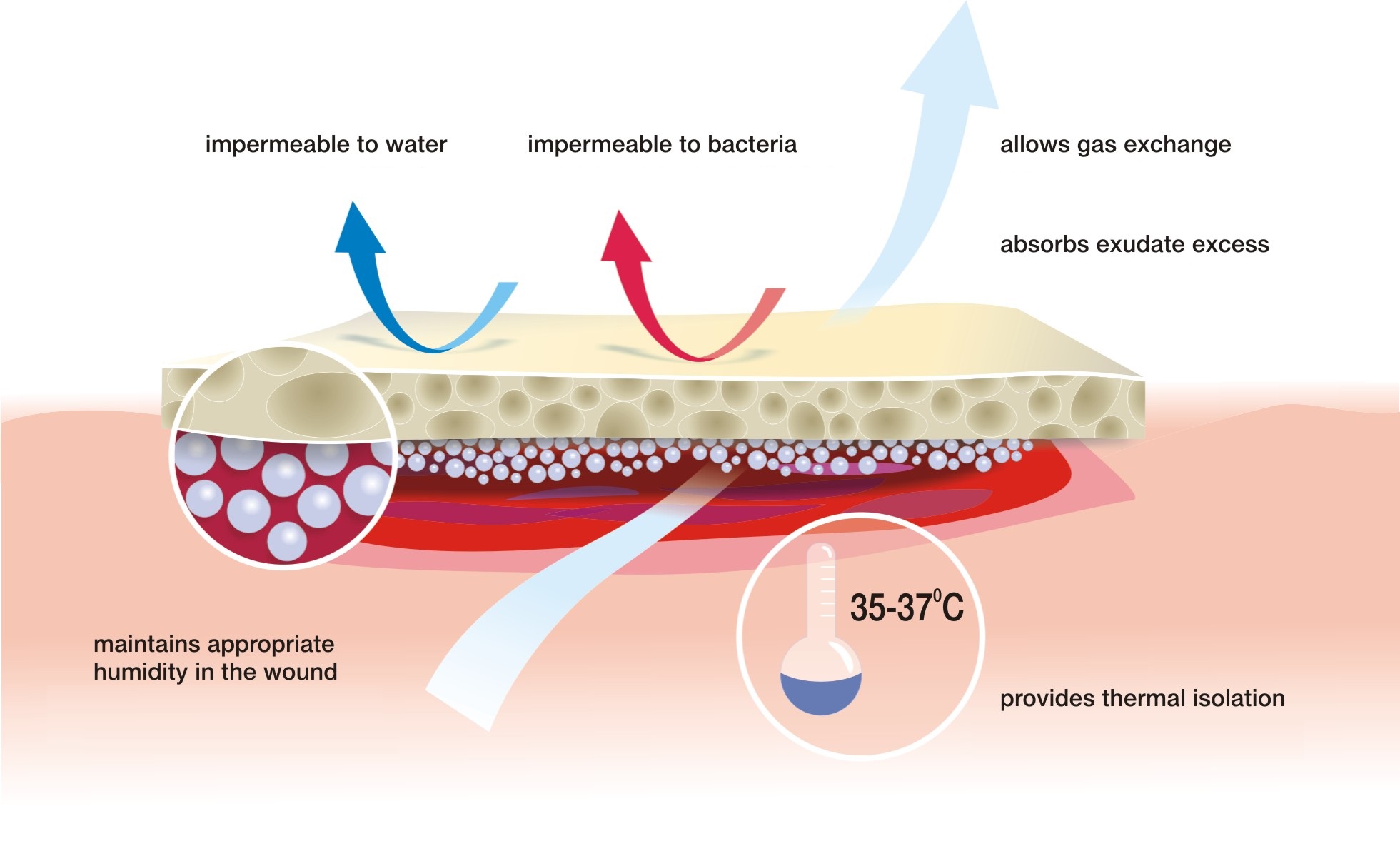
Moist wound healing is most appropriate for hard-to-heal wounds but it can be also used for the treatment of usual cuts, abrasions or scratches.