
Our solutions
No search results
Safe operating suite

The operating room, a special place in the operating suite and throughout the hospital, it must comply with the relevant conditions providing safety for patient and staff – to carry out the operation. In the operating room there should be maintained increased health regime, so that it does not become a place where a patient can get infected. Accordingly, the operating room staff requires to maintain specific discipline, show high expertise and relevant skills.
Contemporary built operating suites have air-conditioned operating rooms, thus eliminating the need to install radiators in such places (habitat of dust and pathogenic microflora). The lack of windows also limits the access of air pollutants (mainly bacteria and fungi).
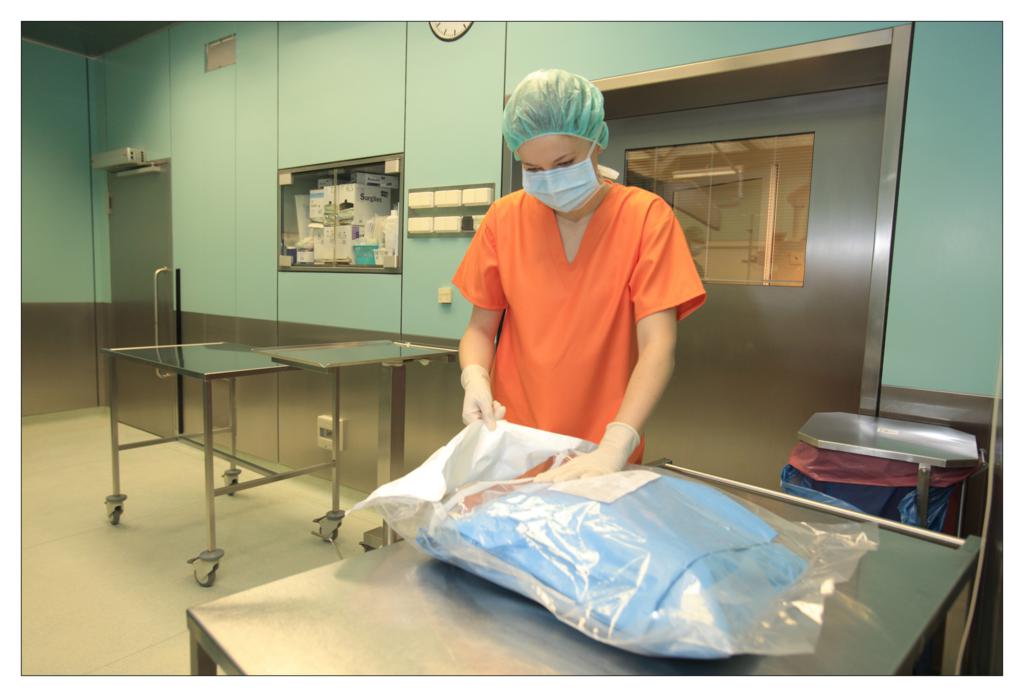
All the operating conditions should be created to safely perform surgical procedures, in accordance with the principles of asepsis. The layout of rooms forming the operating suite should be divided into a dirty, clean, and sterile area and force a one-way movement of staff, patients and sterile material. To ensure the safety of the performed procedure, attention should be paid to all the particular stages, starting with the preparation of material required for the procedure.
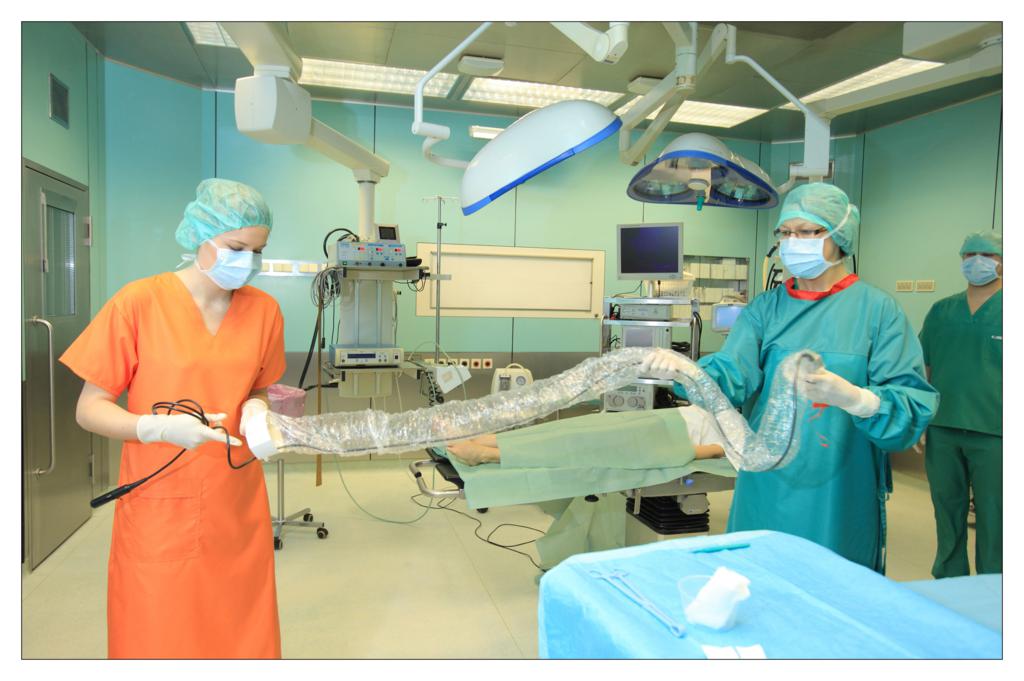
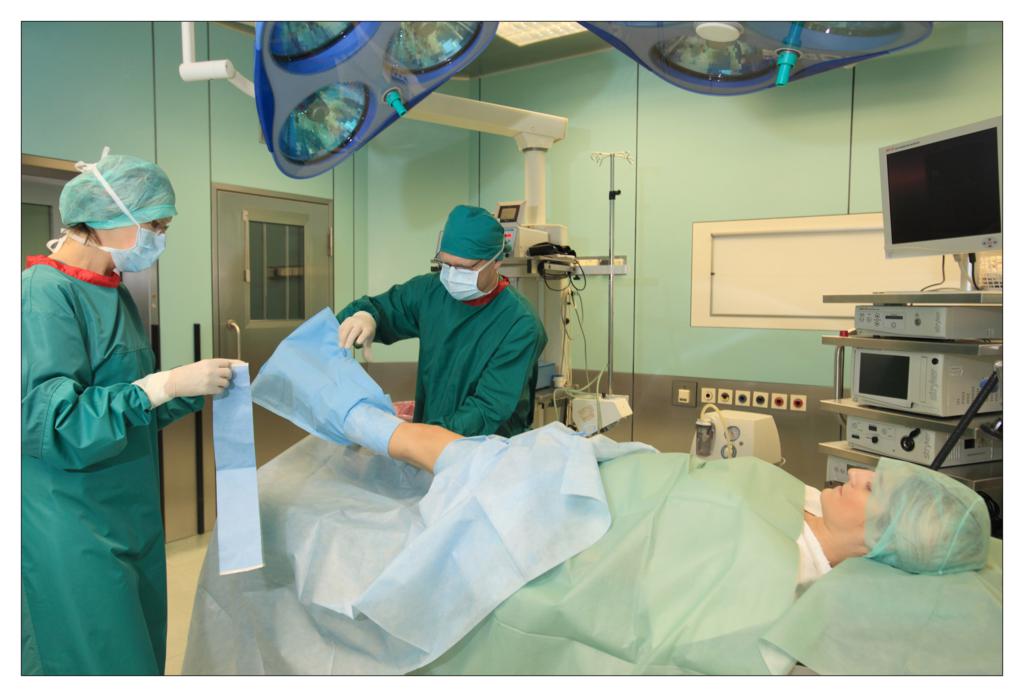
Taking an example of a knee arthroscopy procedure we want to show how to properly protect a patient using the components of the set.
All the used elements are the components of the OP-set.
BEGINNING OF THE PROCEDURE












FINISHING THE PROCEDURE


Caroline Burger
Leiderdorp Hospital, the Netherlands
Saving time, cost control and attention to the quality of care – are key elements for the managers evaluating processes in hospitals. One of these processes is the management of widely understood dressing materials. The solution used in the Leiderdorp Hospital in the Netherlands are so called “custom made” sterile procedure sets. The hospital has used that system for many years.
One of the elements to improve work efficiency in the operating suite is the application of “custom-made” sterile procedure sets, which include all disposable materials needed to perform the surgery, in particular: OP-drapes, gowns, absorbent products and a scalpel. It happens that some special procedures need to be also supplemented with different accessories.

Using a procedure set has many advantages.
- Using procedure sets may contribute to standardise the action mode during an operation. A multidisciplinary team (medical specialists, purchase department, logistics department and manufacturer’s product specialist) determine the optimal composition of the set. When the operating procedure gets standardised, it is easier to coordinate the planning of raw materials according to the action plan in the operating room. In this way, the hospital can effectively manage the inventory, monitor the consumption (which must be compatible with the quantity of performed procedures) and thus reduce costs.
- The use of procedure sets can simplify work for the surgical team. This is important for safety reasons, especially in an emergency, when every minute counts, and the time saving can decide about the patient’s life. It is also important for economic reasons: the possibility to perform procedures in a shorter time means that the operating room can be used more efficiently.
- The management of single sterile components needed to perform a surgery requires a large amount of work. One should indicate not only the time and effort associated with their collection and preparation for a surgery, but most of all work associated with maintaining stock which is safe for hospital functioning. The logistics associated with the management of individual sterile components is far more complicated than the process of logistics related to the management of ready-to-use sterile procedure sets. The simplification of this process increases epidemiological security simultaneously reducing costs.
- An important aspect in considering the advisability of implementing sterile procedure sets is their price. The supplier of a procedure set – because of the scale of delivery – is able to reduce the purchase price of the components. Consequently, the price at which a hospital buys components from a single source must be smaller than the total price of purchased components from multiple suppliers.
- The implementation of procedure sets can reduce the costs associated with the disposal of packaging, which are the reminiscent of the individual components.
In conclusion, the procedure sets simplify all stages of logistics associated with the supply of the operating room in the widely understood dressing material, enable to monitor their consumption, and consequently lead to lower the costs.
Nurse assisting in surgeries at the hospital in Leiderdorp:
I cannot imagine working without the procedure sets. Earlier preparation for an operation was very time-consuming. We had to complete all sterile products, check them, and open one by one. The procedure sets, which we now use are “tailored” to our needs. The saved time we can devote to the patient or perform additional operations. An important advantage is the stable quality of disposable materials. We use disposable drapes, thus eliminating the problem of dusting in an operational environment. Currently, we use six different procedure sets e.g.: for surgical procedures, for surgery of the head, neck and limbs. The use of these specialised sets to me and my colleagues has only advantages.



Manager of the operating rooms, introducing the system of procedural sets in the hospital in Leiderdorp:
As a manager I am always looking for ways to reduce costs and increase productivity. We have analysed the costs of the application of procedure sets and came to the conclusion that the time gained in the operating room directly translates into financial benefits. In addition, we save since the set price is lower and we keep less inventory. We didn’t act rashly, before the purchase we gathered a group of experts to develop a set of wide range of applications. This team with the supplier developed together several procedure sets. They were tested and then, according to our requirements, were adjusted to our needs. The standardisation of the work of all professionals was necessary to ensure the efficient use and broad application of the sets. For this joint effort and commitment were maximally rewarded. The productivity in the operating room has increased and the sets are used with our full satisfaction.
Beata Ochocka
National Consultant for Epidemiological Nursing
In history there are no control groups. Nobody knows what would happen if things went a bit differently.
Cormac McCarthy
Crazy evolution of the virus – “All replicate on the road of dissolution and the subsequent reconstruction” Roland Wolkowicz, a molecular virologist from San Diego State University. “Are we endangered by hunger and epidemics?” – an interview with Joel Cohen, an eminent biologist, a specialist in research on populations. These are just two examples of media reports in recent months. Humanity of the turn of the centuries has many dilemmas and problems, economical, political, these concerning access to clean water and food. These concerns are for nothing since the fundamental problem is, and will be, to protect human health. In the context of the hospital-acquired infections, causes of public health problems include unseen growth of multi-refractory strains, a decreasing number of new effective antibiotics, the lack of vaccines, complex systems of bacteria and virus resistance (MDR XMDR – resistance of bacteria to some or all treatment groups). As the dangerous phenomena of the last decade we must also include winning bacterial biofilms with system “quorum sensing”- somewhat contemporary Enigma cipher. Former “hospital hyenas” return, including Pseudomonas aeruginosa, Acinetobacter baumannii. The result is alarmingly increasing mortality and the incidence of hospital-acquired infections among patients in almost all countries. Claims for infections have become a commonplace element in the functioning of Polish health care and routine activities of law firms specializing in medical cases. The situation in the field of infectious diseases is similarly unfavourable. The old, so-called recurrent contagious diseases (“re-emerging infectious diseases”) returned. An example of anxiety of CDC is pertussis causing, in a global scale, 40 million cases of illnesses and 350,000 deaths annually. At the end of last year, because of the Polio situation, special alerts were declared; the warnings were also made in our country. In 7 countries, including Egypt- so willingly visited by Polish people, there began a massive campaign of additional vaccinations which will target 22 million children under the age of 5. The world is still endangered by “the dirty dozen” of Ebola, cholera, plague, tuberculosis, Lyme disease, and avian influenza.
As the consequence of the development of medicine, including huge progress in the use of surgical and invasive procedures, there appeared hospital infections, HAI.
In these dangerous times of expansion of virulent pathogenic microorganisms, we must ensure hospitalized people with current and highly effective protection against infection, including people undergoing surgery. The history of surgery dates back to the Paleolithic era and runs through the first “operational guidelines of the operating room,” Hippocrates, Galen work, hospitals in shelters and hospices, to achievements of Morton, Bergman, and Mikulicz. Contemporary operating blocks are the most expensive parts of hospitals using sequences of zones of increasing cleanness level. However, it is worth to invest in these areas, in order to obtain the highest possible standards of treatment. In Poland, there have already been applied another ordinance of the Minister concerning the professional and sanitary requirements and developing and implementing of block equipment; to some extent these restrictive regulations impose overcompensating arrears generated in many hospitals throughout the decades of the last century. Prevention of surgical site infections does not apply to a single unit of the hospital: operating block or department. In the case of, both, the department and the operating block, but also in diagnostic laboratories and all the other auxiliary places for those units- there is no room for discretion/arbitrariness in the behaviour of the staff. Hospital acquired infections (HAI) belong to one of the most common clinical form of hospital infections. They are the cause of increased morbidity and mortality of patients, the extended duration of hospitalization, increased treatment costs, damages, but most of all, unfavourable social impacts, such as job loss, including having a great significance consequences of personal distress and suffering of patients and their families.
The history of surgery dates back to the Paleolithic era and runs through the first “operational guidelines of the operating room,” Hippocrates, Galen work, hospitals in shelters and hospices, to achievements of Morton, Bergman, and Mikulicz. Contemporary operating blocks are the most expensive parts of hospitals using sequences of zones of increasing cleanness level. However, it is worth to invest in these areas, in order to obtain the highest possible standards of treatment. In Poland, there have already been applied another ordinance of the Minister concerning the professional and sanitary requirements and developing and implementing of block equipment; to some extent these restrictive regulations impose overcompensating arrears generated in many hospitals throughout the decades of the last century. Prevention of surgical site infections does not apply to a single unit of the hospital: operating block or department. In the case of, both, the department and the operating block, but also in diagnostic laboratories and all the other auxiliary places for those units- there is no room for discretion/arbitrariness in the behaviour of the staff. Hospital acquired infections (HAI) belong to one of the most common clinical form of hospital infections. They are the cause of increased morbidity and mortality of patients, the extended duration of hospitalization, increased treatment costs, damages, but most of all, unfavourable social impacts, such as job loss, including having a great significance consequences of personal distress and suffering of patients and their families.
The occurrence of infectious complications related to the surgery on which we have influence, can be effectively constrained and reduced to a safe level.
Among others, through the proper hygiene of the treatment environment, hygiene of the patient being treated, following the anti-epidemic procedures in surgical departments and treatment rooms, personal hygiene and the use of appropriate peri-operative preventive measures and all other activities in the sphere of protection of surgical site against infection. During the budgeting period it is worth to spend a larger part of the hospital funds on the hygiene and prevention of hospital-acquired infections. Money spend in this way will bring profit.
The latest data on hospital infections comes from a European spot survey made on the EU member countries and from Croatia, additionally conducted in 2012. It is published by the report of European Centre for Disease Prevention and Control, ECDC. The study assessed the overall prevalence rate of infections associated with healthcare in Europe at 6%. Poland received slightly higher percentage – 6.4%. The base of the entire study were information taken from 947 European hospitals. Our country illustrated the data from 36 hospitals that meet the criteria of the protocol; most numerous in the study were provincial and specialist hospitals – 27.8%, clinical and highly specialized – 19.4%. In Europe dominated clinical hospitals – 31.8%. The number of patients in the study was over 231,000, including Polish patients – more than 8,000. In my opinion, it is an interesting fact that more European than Polish patients were taking antibiotics – 35% vs. 31.9%. European treatment departments received the level of infections above the overall average for SSI – 6.9%. Polish treatment departments received a result below 6% of general and treatment morbidity – 5.6%. For the most common clinical form of hospital infections, hospital-acquired infections ranked in second place after pneumonia (Europe 19.6% vs. Poland 20.2%). The difference between these two figures was low- 0.2% .The bigger differences between European and Polish data concern infections in paediatric departments.
Reports from Polish research centres in recent years illustrate the importance of the HAI problem in patients undergoing surgery. The two-year study of Giedrys – Kalemba on a population of nearly 300 kidney recipients in Western Pomerania proved that it is a very important clinical problem in transplantology. In this study, surgical site infection, which was diagnosed in patients after kidney transplantation, was located in a third place with a rate of 7.6% in researched clinical centre and 12.9% in the hospital of the provincial rank. It should be noted that an increasing number of branches engaged in organ and tissue transplantation environment devoid the natural micro flora.
Document of the European Centre for Disease Prevention and Control, ECDC, describes in detail definitions of surgical site infection (HAI, SSI). They were developed by an international group of experts in 2009, in order to unify criteria for diagnosis of infections as part of their monitoring, in all European Union and cooperating countries. They are mainly based on IPSE / HELICS definitions used so far, and supplemented by definitions of the US CDC infection of the newborn. In the range of SSI definition, there were highlighted and described in detail: superficial infection at the incision site, deep incision site infection and infection of the organ / site. Recognition of these cases is based on the criterion of clinical symptoms, isolation of microorganism and the appearance of the symptoms.
It is confirmed that the risk of SSI prevalence is correlated with the risk of the procedure and depends on the patient’s general condition. Illustrating the likelihood of SSI for the same treatment in a patient with low risk – in a patient at high risk, it may even be several times higher. The literature states that the incidence rate of infections after surgery in the clean site is approximately 2%, in the dirty, infected zone it may reach above 30%.
Infection control is the basic standard for the proper care of hospitalized, operated patients.
The program of infection control at the surgical site should include the study, control and analysis many of the issues carried out in cooperation with numerous departments of the hospital: the technical, functional and sanitisation conditions, organization of work, shortening the length of stay of the patient in the hospital before surgery, the implementation of a set of basic steps to prepare a patient for surgery, system of supervising and monitoring adherence of hand hygiene, asepsis and antisepsis, proper planning of procedures, prophylactic use of antibiotics, targeted antibiotic / antibiotic therapy, level of insulation, active monitoring of infections and alarming factors, continuous training courses, hygiene of ward, dealing with underwear and medical waste, profession control, immunization and health surveillance of the personnel correspondingly with the requirements of use of medicinal products and medical devices.
To the factors enhancing the risk of hospital infections of surgical site, mentioned at the beginning of the article, there should also be included decontamination challenges: cleaning, disinfection and sterilisation of specialized equipment in surgical wards. Procedures for medical, nursing and assistance proceedings undergo very dynamic changes. On one hand, changes generate progress, provide access to effective and rapid treatments, on the other hand, new technologies and materials for treatment, such as: implants, wound dressings, drainage system, skin disinfection, surgical techniques, improperly applied and decontaminated medical devices may be source for undesirable events.
In every surgical ward, each instrumentalisation favours infection, and the action performed aseptically reduces the risk several times. Another important cause of infections in patients undergoing treatment is the repeated interruption of natural skin-mucosal barrier. It is very dangerous and conduces a high risk of haematogenous infections. Vascular lines, nutrition, parenteral nutrition, tests … the gates of dozens of potential infections. How much knowledge about infections and concern is needed of people working in surgical wards! But treatment and care are not only on an outpatient basis, but also elements of psychology, “healing with words”. One of the basic, reliable principles of infection prevention was, is and will remain, hand hygiene. This is the easiest method of preventing surgical site infections for their most common cause is the transmission of bacteria between patients on the hands of staff. Hand hygiene must be understood in a complementary way, which means applying to all but the staff, patients and visitors, including a hospital chaplain, lab assistant, radiologist, nutritionist, trainees and students. For over a year, in Poland, there is a WHO campaign, promoted by many individuals and institutions, which is aimed at raising the discipline of obeying cleanness of hands in medical facilities “Clean care is safer care”. Hospitals are counting the amount of consumed resources, held conferences, actions and appeals. These are needed, but I hopefully anticipate time (organically, working in the field of education at basis) when this cheap and simple habit will be instilled in our professional credo as a natural reflex, without which we will not perform specific tasks at patient and in the treatment environment both closer and further.
The presence of various resistant strains of bacteria in the aetiology of surgical site infections requires sound knowledge and proper control by the hospital Infection Control Team. However, it should be required from the entire therapeutic team, led by department manager sensitive to the issue of hospital infections, physician in charge of the patient, to recognize the infection rapidly, early implemented therapy based on antibiogram and widely understood cooperation with epidemiology specialists. There are no such hospitals in the world where their good hospital flagship will have a zero rate of hospital-acquired infections. This situation is not acceptable! This is a bad flagship. Hospital infections have been, are and will be an inevitable concomitant component of treatment, especially hospitalization, treatments. But they must be minimized, controlled. Polish epidemiological nursing, not only in my opinion, has achieved so much success and has contributed most effectively to change the image of the fight against infections in the last fifteen years, co-creates modern model of infection control. There’s a place for everyone. These successes bring more joy, because in no fully satisfactory economics of hospitals, the introduction of verified in other countries facilities and solutions – is much more difficult. In my opinion, the current treatment procedures include those solutions and, what is most important, these procedures work in practice. All records are now proceeding algorithm for clinicians, but in the context of infections, proceeding in accordance with the procedure confirms the concern for patient safety. One of the world’s most widespread assessment of the patient state before surgery is the scale of ASA. It punctuates health depending on the basic disease and the clinical condition; studies show that the results of measurements conducted by its use correlate with the incidence of SSI. The more risk factors, the higher risk of complications and death of the patient. The image of contemporary infectiology causes that the surgeon has contact with microbiological challenges beside the therapy and diagnostics.
Infectious complications significantly delay recovery of the patient after the surgery performed. Microbes colonizing the skin and mucous membranes of the patient are a serious source of infection.
Nearly half of infections after surgery in the clear area is the result of contamination of the patient’s own flora. The risk of SSI increases due to the presence in the body of the patient dangerous inflammations and trans-located by haematogenous way of bacteria to the wound. A significant problem in surgical patients is carriage of Staphylococcus aureus strains, an emergency situation is the finding in a patient MRSA resistant strain. Determined with the presence of hospital epidemiologists, groups of patients (recipients of organs, patients with large deficits of immunity, long-term antibiotic therapy, being under the long-term care and ICU, others with a high index of risk of infection) should be monitored and diagnostic material should be taken at the time of admission to the ward or before the scheduled admission in order to carry out decolonization. These include: eradication of nasal part, decontamination of the body, the use of isolation as a primary means of protection against cross infections and dangerous for surgical wards epidemic outbreaks, which can quickly hinder or prevent the normal rhythm of ward’s work. Recent studies have shown that the benefits of simple and inexpensive procedures of decolonization is more effective than previously thought in comparison to the administration of drugs, including vancomycin. Another warning should be added. At the end of last year, very disturbing information started to reach the Polish epidemiologists about the significantly high percentage of MRSA infections in Polish hospitals in recent studies. So, another “hospital hyena” shows its merciless face, and MRSA remains one of the most important factors that cause surgical site infections. Considering the SSI subject a significant problem for surgery, concerning infections caused by Clostridium difficile, should be signalised, which main reason is, among others, antibiotic therapy. Each diarrhoea must be diagnosed. Part of the patients treated in surgical wards meet the criteria for the development of this infection; it is important for the personnel’s conduct to be marked by strict obeying of the regime against the risk of environmental contamination of spores. CDI accompanying patient after surgery significantly impairs the healing process. In 28% of patients with primary infection with Clostridium difficile, relapsing can be observed.
Reducing the risk of developing SSI
In this part of article about so invariably important problem for operated patients, their families and for us- physicians, fulfilling and supporting from different parts the safe process of a patient’s stay in hospital, there is an opportunity to remind few aspects of the recommendations of reducing the risk of developing SSI, which I gave in my opinion as a national consultant in 2010:
- in the day preceding the surgery and the day of surgery, prepare the patient’s skin by bathing the whole body with the use of professional antiseptics,
- for patients with confirmed bacterial colonization or infection caused by methicillin-resistant Staphylococcus aureus, skin decontamination should be carried with means of proven efficacy biocide,
- in the day of surgery, under general anaesthesia, on a patient should be carried out disinfection of the oral cavity with the use of a professional antiseptic to reduce bacterial bio film,
- if the hair cannot be left around the cut site, preoperative hair removal should be performed in the shortest possible time from the beginning of the surgery with the use of cutting or depilatory methods (blade must be used once),
- for surgical procedures, clothing and barrier materials should be used,
- principles of perioperative antibiotic prophylaxis should be strictly abided,
- the number of people in the operating room should be limited,
- in the ward and the operating wing aseptic and antiseptic rules should be absolutely abided,
- medical devices should be used in accordance with rules and the rules of sterility of products and how to use them should also be abided
Introduction to surgery the techniques for minimally invasive surgery (MIS), robotisation, peri-operative medicine concepts, the idea of an integrated operating wings, allows surgeons to use their skills with intensified strength and personnel for more comfortable work. Will it be enough to deprive the patient of adverse consequences, complications, and above all, to eliminate or reduce SSI? In my opinion – no. Knowledge, diligence and conscientiousness of the staff are the basis for effective prevention of hospital infections. In infection control, abidance of recommendations is a key to success, into which also patient and his family should be involved. In the surgical wards invaluable are the procedures for hand hygiene, catheter related infection, peri-operative prevention, proceedings towards a patient with KPC, MRSA and Clostridium difficile. Polish Association of Epidemiology Nurses in its scientific notebooks and quarterly “Nurse Epidemiology” refers to many aspects of protection against hospital infections concerning the medical staff, these positions are available and can be a very good and reliable complement to treatment clinical knowledge.
At the end…
What complicates the risk situation? It might be worth to look at this meaningful list, to which once again from many years the history of infections added another verses:
- overpopulation and easier migration between countries,
- aging of the population, immunological disorders,
- gathering of people exposed (the flow of patients in hospitals),
- resistant bacterial pathogens,
- overcoming barriers between species,
- lack of medical personnel.
- drug abuse and antimicrobials (selection of resistant strains)
- invasiveness of medical procedures.
- substitution of animals, food, plants,
Waiting for “miracle drugs” such as what once was penicillin and subsequently occurring after them therapeutics, we shall accept with humility the principle that at this stage of treatment we favour the principle of “cleanness reasserts us health, and our patients….” and necessarily follow the instructions and medical procedures preventing infections!
Literature:
- Deptuła A. Pierwsze ogólnopolskie badanie występowania zakażeń związanych z opieką Zdrowotną i stosowania antybiotyków( EU-PPS HAI&AU) – różnice pomiędzy Polską a Europą, Kraków: XX Zjazd PTZS; 2013
- Giedrys – Kalemba S. Zakażenia u pacjentów po przeszczepieniu nerki – doświadczenia własne Kraków: XX Zjazd PTZS; 2013
- Izydorczyk E. Praca pielęgniarki na bloku operacyjnym, Magazyn Pielęgniarki Operacyjnej 8/2013
- Bober – Gheek B, Fleischer M Podstawy Pielęgniarstwa Epidemiologicznego, Warszawa: CKPPIP; 2002
- Definicje zakażeń związanych z opieką zdrowotną (HAI), ECDC, NPOA, www. antybiotyki. edu.pl
Miroslav Hricišák, MD
A doctor in charge of a same-day medical care unit
Euromedix a.s., ProCare Polyclinic
Betliarska 17, Bratislava
Over the 21 years of my surgical, outpatient care and operating practice, I have worked in many places and there I developed certain work routines and the habit of using proven procedures. As time went on and my experience grew, I worked to improve the procedures, switching to less complicated and more cost-effective working methods whether in outpatient surgery departments or in operating theatres.
After leaving my previous employer, I took on the challenge of building a new outpatient surgery department at the polyclinic and a same-day medical care department specialising in surgery and orthopaedics and, some time later, gynaecology, plastic surgery, urology, and head and neck surgery.
At first I thought that the work would be fairly easy and that I would be able to make use of what I already knew or would learn, and that all other things would come easily somehow.
 The first step was, together with my team, to decide what products we would need. After that, we contacted a number of suppliers to share our ideas and requirements with them. There were, of course, certain limitations, such as the space at the polyclinic premises, a tight budget, the scope of activity or logistics, I had to change my point of view and, in the setup process, make use of many established procedures and routines. My ambition was to develop a model as simple and cost-effective as possible.
The first step was, together with my team, to decide what products we would need. After that, we contacted a number of suppliers to share our ideas and requirements with them. There were, of course, certain limitations, such as the space at the polyclinic premises, a tight budget, the scope of activity or logistics, I had to change my point of view and, in the setup process, make use of many established procedures and routines. My ambition was to develop a model as simple and cost-effective as possible.
One of the key decisions relating to the operating theatres was the choice of OP-drapes. Should we use a laundry or go for disposable surgical drapes and linen ?
In the outpatient surgery department, I tried the small disposable operative sets made by TZMO SA. At first, I was sceptical about using materials that were new to me and that I had never used before. After some time, however, the outpatient operative dressing sets, the tissue sample collection sets or catheter placement sets became my favourite products. The preparations for surgical procedures and the procedures themselves took much less time now.
At the same-day medical care unit, I used different operative sets made by TZMO S.A. specifically for different surgical and orthopaedic procedures. After many surgical consultations and discussions with TZMO S.A., the manufacturer provided us with “made-to-fit”, large operative sets containing sterile disposable OP-drapes, such as patient drapes, instrument table covers and surgical gowns. We also ordered some accessories, which were also made and packed on a custom order basis. The sets contained sterile items, such as different dressings, bags, self-adhesive pockets for liquids and medical equipment, plus tampons, bowls and elastic bandages.
The operative sets also contained disposable metal instruments (scissors, tweezers etc.), but I haven’t been using these instruments for long enough to say what I think of them.
We liked the operative sets supplied by TZMO SA so much that after three months of working in the same-day medical care unit, we discontinued using materials from other suppliers.
Being a small team, we are doing our best to perform the largest possible number of surgical procedures in the shortest possible time. Large operative sets help us reduce the time needed to prepare our operating theatres for procedures. Also, when we need to replace our surgical nurses with external surgical personnel, the risk of failure due to different working habits is none. The large operative sets designed for specific surgical procedures have made our work easier and improved the safety of our patients and our personnel.
The operative sets also contained disposable metal instruments (scissors, tweezers etc.), but I haven’t been using these instruments for long enough to say what I think of them.
We liked the operative sets supplied by TZMO SA so much that after three months of working in the same-day medical care unit, we discontinued using materials from other suppliers.
Being a small team, we are doing our best to perform the largest possible number of surgical procedures in the shortest possible time. Large operative sets help us reduce the time needed to prepare our operating theatres for procedures. Also, when we need to replace our surgical nurses with external surgical personnel, the risk of failure due to different working habits is none. The large operative sets designed for specific surgical procedures have made our work easier and improved the safety of our patients and our personnel.

With standardised surgical procedures, the risk of errors and, consequently, the possible complications is reduced. The post-surgery cleaning and material removal jobs are now much easier, which gives us more time to prepare for the procedures that follow. The central sterile services department personnel no longer have to sterilise surgical materials, as these are supplied sterile by the manufacturer. As a result, the surgical nurses can focus on the surgery itself. The standardisation of procedures through the use of large operative sets offers economic benefits too. Normally one set is used during one surgical procedure, meaning that there is practically no waste (unused materials). Keeping records of the use of the materials is easy – the material labels with codes are inserted in the files for archiving. This helps to calculate the actual costs of procedures. The costs of the personnel involved in the storage and processing of surgical materials are also reduced.
After my experience of using small and large operative sets at the polyclinic and the same-day medical care unit, I would never switch to other solutions.