
Our solutions
No search results
Outpatient clinic
Working in the treatment room is fraught with high risk of infection, which can be caused in various ways. One of them may be bacterial contamination of instruments, equipment and surfaces used in the course of the procedure. The danger in particular way may relate to the equipment which penetrates into sterile body space. To prevent the spread of infections, it should be ensured that the used instruments are sterile. This requirement applies to all instruments used in the procedures connected with tissue discontinuity, or requiring contact with the mucous membranes or damaged skin, e.g. dressing change or removal or application of sutures. In a situation where re-usable instruments are applied, we are forced to make costly sterilisation process to prepare them for reuse.
Another type of problem is secure collection of infected waste generated during the procedure. Due to epidemiological reasons we are forced to keep them in specially designated containers in accordance with accepted for this type of material rules. In particular sharp instruments should be disposed of with great caution.
A great help in simple procedures is the use of ready-made sets dedicated to perform a specific medical procedure. The set content and their form enables to easily conduct the procedure at any time preserving all security regimes relating to both the procedure itself and the safe storage of contaminated material generated during the procedure.
The advantage of the sets is the safe way to store all the needed materials and their readiness to be used at any time.
The photos present an example of a suture removal procedure with the application of a special dedicated set.
Disposable metal instruments are hazardous waste with sharp ends and edges which are to be collected in durable containers, resistant to moisture and chemicals, with the possibility of single closure.
SET COMPONENTS

COURSE OF THE PROCEDURE




The word ”end” means not just the end, but also the goal. In Polish the ”end” is rarely used as the goal, and more can be associated with the closure of one stage and the start of a new and different one from the current reality. Thinking straight the end is a new beginning i.e. changes.
Changes are often associated with fear and temporary difficulties, which people are not always ready for. The need to leave the safe and tame zone always causes fear of what will happen.
If the proceedings are recorded in the medical procedure, the change of this action seems to be very difficult and unreasonable, because the current performance of procedures was effective and unchanged for many years. However, it often happens that the change involves a number of positive consequences, and thus modification of the previously stable reality in a very positive way.
The effects of changes associated with the introduction of ready-for-use-sets and the benefits resulting from that are discussed by:
Emilia Zawadzka
Master of Nursing with specialisation in epidemiological nursing – Dr. Władyslaw Biegański Regional Specialist Hospital in Grudziądz
Monika Cerkaska
MatoNews interviewer
Monika Cerkaska: Why did you decide to work with specialist sets? Is it only because of the relief for the Central Strerilisation Unit?
 Emilia Zawadzka: From the moment the CSU started to support 11 operating rooms, we decided to use it only for the sterilisation of instruments. Relieving the work of CSU we resigned from creating sets of dressings material inside the hospital and decided to use sterile procedure and operative sets. I am thinking of ready-for-use sterile products, in a single package containing both the dressing material, Op-drapes and other components needed to perform a particular procedure. In this way the responsibility for the sterility of the material is transferred onto the manufacturer, and the CSU can focus on the preparation of sterile surgical instruments.
Emilia Zawadzka: From the moment the CSU started to support 11 operating rooms, we decided to use it only for the sterilisation of instruments. Relieving the work of CSU we resigned from creating sets of dressings material inside the hospital and decided to use sterile procedure and operative sets. I am thinking of ready-for-use sterile products, in a single package containing both the dressing material, Op-drapes and other components needed to perform a particular procedure. In this way the responsibility for the sterility of the material is transferred onto the manufacturer, and the CSU can focus on the preparation of sterile surgical instruments.
Due to such a decision, a large work load relief was also felt by nurses who were expected so far to prepare sets of dressing material. Not only the work comfort increased, but also ensured our and patients’ safety. The use one set specifically designed for a given surgical procedure eliminates the risk of error and thus minimises the risk of complications. In addition, the time devoted to prepare all the necessary materials for the surgery is much shorter, which is especially important in life-saving situations.
The use one set specifically designed for a given surgical procedure eliminates the risk of error and thus minimises the risk of complications.

M.C.: What kind of response from the doctors and nurses, the direct users of the sets, did you meet while changing into ready-for-use sets?
E.Z.: Any change or introduction of a new solution causes some concern among those who are directly affected. So it was in our case. Both among the doctors and nurses there were concerns that quickly disappeared when they started working with the sets. We all experienced better working conditions, and today we cannot imagine return to the previous state. It is much easier and safer to open one set than a few products in aseptic packages. While opening one package, we reduce the possibility of contamination of products and patients with pathogenic microorganisms. In high-risk procedures with high risk of complications the elimination of errors translates into patient’s safety, which is the most important thing for us.
M.C.: Which elements of the set are the most important for you?
E.Z.: First of all, the set should be complete, but not exaggerated. Unused elements constitute waste, for which, unfortunately, you would need to pay. Therefore, the most important are the basic elements, which if necessary can be supplemented with sterile material. In an emergency, when there is time pressure, it is important that the set contains everything necessary to carry out the procedure.
An important advantage of the product in the form of the set is the fact that the order of arrangement of individual elements can enforce the execution of particular activities, e.g. first the instrument table is covered, the OP-field is disinfected and secured in the right way. These are the activities which are always followed one another, and the order in which they appear has a big impact on the safety of the procedure.
M.C.: What about human habits? Do they not induce resistance to the use of medical devices in such a form?
E.Z.: The procedure should be carried out in a safe manner and habits should most of all provide the security. I do not see any conflict of interest.
Speaking of safety one must also think about legal security when a patient can claim against the hospital, like in the case of medical incidents. The awareness of patients is increasing, the affairs between the patient and the hospital quickly become media events, and each won process generates another claim. Therefore, it is important to have evidence that all the procedures in the treatment of the patient are carried out in a secure way. Medical records are proof in this case, which are facilitated by a TAG label i.e. stickers that can be stuck into the patient’s medical history and the documentation of the operating theatre.
M.C.: Which arguments do you think are stressed by the hospital manager?
E.Z.: I’m sure that epidemiological safety and costs. The cost reduction and of course the set price is very important, and for the director / manager the transparency of costs. The set price is equal to the real cost for the ward for the performed procedure. We are talking about a simple ratio: the number of sets is equal to the number of performed procedures. In this case we eliminate the so-called hidden costs and limit the possibility of manipulation of the costs of individual procedures.
M.C.: The economic aspect is a very strong argument. What about work ergonomics in the ward? Is it changing?
E.Z.: Of course. It great relief is felt by the personnel. Workload for nurses is very high, and in a situation where we use ready-made sets, all the energy is focused on the patient.
In addition, the use of sets streamlines logistics inside the hospital. Products are transported easier and safer.
M.C.: Thank you very much for your time.
Dr. Władyslaw Biegański Regional Specialist Hospital in Grudziądz has 40 wards, in which there are 1,050 beds and 53 specialised outpatient clinics. Modern operating theatre has 11 operating rooms supported by a Central Sterilisation Unit (CSU). Due to the large relief for the functioning of the CSU the hospital has completely changed the approach to purchase management of products for the greater use of ready-made sterile procedure and operative sets and the transition from reusable to disposable products.
Within the European Regional Development Fund the hospital acquired also funding for the purchase of new ambulances with equipment, for the construction of one of the most modern heliports in Poland and for a wide range of medical equipment that is used in the treatment of patients in the new clinic.
The use of large operative sets in the operating theatre of the Nicolaus Copernicus Provincial Specialist Hospital in Łódź are discussed by:
Sylwia Dąbrowska
Deputy Head of the Operating Theatre for Nursing – Nicolaus Copernicus Provincial Specialist Hospital in Łódź
Monika Cerkaska
MatoNews interviewer
Monika Cerkaska.: What urged you to start working with ready-made sets?
Sylwia Dąbrowska: The decision to introduce the standard use of disposable sets in the operating theatre happily coincided with the renovation of the operating theatre. Once, that is before the renovation, within the operating theatre we had a sterilisation unit, where in addition to current work for the needs of the theatre, there were also sets of non sterile materials prepared that in the next step were sterilised. After the renovation of the operating theatre, the sterilisation unit was closed and today the hospital has only a delivery and receipt point dealing with logistics, mainly of instruments and hospital clothing. Due to such a decision at one time we started to use disposable products such as surgical drapes, gowns and procedure or operative sets.
The renovation of the operating suite also reduced the size of storage space that we have. Therefore, we cannot afford to maintain a very large stock of non sterile products, which always occupied a lot of space. Nowadays, we use a very large number of implants, and they mainly take place in the operating room. Dressing materials are stored outside the operating room, and therefore it is easier and safer then to use a ready set. Such an organisational approach is very reasonable. Reducing the storage space, the space for the patient increases. And this is of course connected with money.
One move is enough to open the set, one set designed for a given procedure, and one label that allows the transfer of information to the documentation highly limit the time devoted to prepare for a surgery. This allows the medical staff to concentrate on their work around the patient.

M.C.: You mentioned the safety. It’s probably one of the most important reasons for the hospital, for which you have decided to work with the ready-for-use product?
S.D.: Of course, and it is for the hospital as a whole. This is a very strong argument for the manager – because the responsibility for sterility lies with the manufacturer – and for the entire epidemiological staff – for the use of sets reduces the number of hospital-acquired infections. It is also very important for us – as the medical staff. It is safer to open one packaging rather than opening individual packages of products needed to complete the procedure. The removable part of the label is a very safe element. To eliminate the error, which can be committed in the process of rewriting the data into the documentation, in this case only one sticker with a product code and expiration date is transferred. The product code fully identifies the contents of the package and there is no need for a more detailed label. At the big amount of material used and also having a limited amount of place in the documentation, the size label is adequate.
Another advantage of using the sets is to increase work comfort. One move is enough to open the set, one set designed for a given procedure, and one label that allows the transfer of information to the documentation highly limit the time devoted to prepare for a surgery. This allows the medical staff to concentrate on their work around the patient This is especially important in a situation where for example on call there are three operating rooms functioning, and there is just an enough number of nurses to do the work on the ward. Using the finished product allows for smooth work throughout the operating suite on duty. Of course, the comfort of using the sets is experienced not only in emergency situations, but also in our daily work. We minimise the duration of the procedure, which translates into individual savings, i.e.: lower consumption of energy and air conditioners, shorter anaesthesia, shorter work of a surgeon, anaesthetist and nurses. Minimising the time devoted to the preparation for a surgery, combined with efficient team work makes the performance of the procedure faster and cheaper.
M.C.: The cost is still to be discussed, but yet another question arises. Do I understand it correctly that the work with the sets increases the efficiency of the operating room?
S.D.: By all means yes. In addition to the mentioned sets also the high quality of disinfectants that allow for very rapid turnover of patients in the operating room contributes to better efficiency. Taking our hospital into consideration, I can say that until recently, daily we performed four procedures e.g. strumectomy. Today we can perform five operations and we have still some reserve time. This shows the efficiency and getting in sync of the team, as well as shorter time devoted to prepare for a surgery. This is most noticeable while analysing the productivity of the operating suite for a month or a year.
M.C.: Yet another question about the waste. Can we assume that the amount of waste gets reduced?
S.D.: It depends. Generally, the amount of medical waste coming from the operating theatre increases. This happens in all medical units using disposable products like disposable OP-drapes, medical devices, gowns, etc. However, the amount of waste, in the case of unit packages of the products used during the treatment certainly drops and is limited to a few, and not as it once was – a dozen or even dozens.
M.C.: So how do the costs of a procedure change after implementing disposable ready-for-use sets?
S.D.: I have no doubt that this solution is far more profitable for the hospital, because we have a finished and adjusted for our needs set, sterilised and delivered. Completing components inside the hospital in our reality would involve an additional job position, and that means an increase of the cost of the procedure. The best and the most advanced solution are sets dedicated for a particular medical procedure. This reduces not only the amount we opened dressing materials, but also in such sets you can find OP-drapes, a Mayo table cover, covers for equipment and cables, organisers for the equipment used during a surgery – a very useful and work ordering thing i.e. a whole load of sterile material. In this case, the cost of the given procedure is countable and very readable. The number of performed procedures is equal to the amount of used sets.
M.C.: Thank you very much for your time.
Nicolaus Copernicus Provincial Specialist Hospital in Łódź in its complex structure has: Specialist Hospital, Regional Oncology Centre, Dr. Janusz Korczak Paediatric Centre, Group of Clinics and Specialist Clinics as well as Diagnostic Department.
The biggest success for the hospital was the creation of the Bone Marrow Transplant Centre managed by a specialised team of experienced scientific and technical staff, and the creation of a Hospital Emergency Department integrated with a heliport forming a functional unit guaranteeing rapid rescue in life threatening situations. An important achievement was the modernisation of the Regional Oncology Centre.
Currently, the hospital provides comprehensive diagnosis and treatment at the highest level, thus providing conditions for faster patients’ recovery.
In the hospital there are also 12 associations and foundations supporting inter alia patients with cancer, leukaemia, haemophilia, rheumatic diseases, a heart transplant, and many others.

Nosocomial infections are a major problem in modern medicine, because many times they are mean a failure in the treatment and the emergence of complications. The most common problems associated with infections is the lack of aseptic behaviour in the where a medical procedure is performed, a delay in the diagnosis of infection or improper treatment. For the hospital, it is connected with the fact that all these aspects – prevention, diagnosis and treatment – must be done properly.
More and more hospitals decide to obtain an ISO certificate, which leads to the development of procedures for all phases of patient treatment, the observance of which will reduce the number of infections. Moreover, the awareness of the medical staff of this problem is increasing year by year.
The problem of nosocomial infections is also a challenge for manufacturers of medical devices used in the performance of specific procedures in health care units.
The answer to the security needs of the treatment are Matoset products that combine functionality and economy by intentional combining of dressing material. In other words, the individual Matoset is dedicated to a given medical procedure, and particular elements are arranged in a way forcing to perform activities in a particular sequence in accordance with asepsis principles. The structured arrangement and thoughtful composition translates to security, convenience and time saving.
Interview:
Monika Cerkaska – TZMO Product Manager
Katarzyna Moś – Master in Nursing with a specialisation in epidemiological nursing
M.C. In which situations the use of sterile Matoset sets worked best?
K. M. In our daily practice we use Matoset products mainly in treatment rooms, when we have to perform minor medical procedures, such as suture removal or dressing change. Using the sterile sets I am sure that I have all the necessary materials prepared and within a few moments I am able to perform a minor procedure. The ready-for-use sets are indispensable at the patient’s bedside when transporting the patient and performing a procedure in the treatment room is not possible.
M.C. And what about situations when you need to change the dressing at patient’s home?
K. M. Exactly. The health visitor will surely appreciate the comfort of using the sets. It is always certain that all necessary materials are prepared, and each patient has a sense of individual treatment and safety guarantee since the set is designed specifically for him.
M.C. So it much easier to work with the set?
K. M. Yes, it’s easier because they improve the course of a medical procedures, but also thanks to them the work is a lot safer. The arrangement of particular elements determines the actions to be performed. We cannot omit any items e.g. gloves, which are usually placed at the top, and only after their application it is possible to use other sterile components. This minimises the risk of infection, and this is important both for us and for the patient. The documentation process is facilitated by adhesive labels with information about the product, which can be placed in the patient’s records.
M.C. So can we conclude that the sets guarantee the asepsis regardless of the place of performing the procedure?
K. M. Yes, we can. The patient is not always in a place where it is possible to e.g. securely change a dressing. Matoset enables us to do so, and also reduce the time to prepare for the procedure and facilitate the organisation of the work.
M.C. At the end I have to ask – what about the costs?
K. M. The application of complete sets dedicated for a given procedure eliminates the need to open multiple unit packaging, which directly translates into the cost of the procedure. When you open a few packs it increases the possibility of infection of the sterile material. Besides, using the sets – all the content is deliberately used. The rational use of dressing material certainly reduces the cost of its purchase. In addition, medical staff does not have to devote time to complete the dressings for the procedure. In conclusion, I would like to add a few words about the catheter sets and sets for the disinfection of the surgical field, which will surely work well in emergency rooms, although, of course, not only. In situations where time counts, we are not always able to fully observe aseptic rules, the lack of which – as you know – can lead to complications and the cause of prolonged hospitalisation. A patient who is in a life-threatening situation requires undertaking multiple procedures at the same time. The risk of infection while saving lives is greater than during the planned procedures. Therefore, the use of Matoset in the form of ready-for-use sets, such as the catheter set helps to observe the asepsis. A set that contains all the necessary components including an adequate size catheter, allows for the reduction of unnecessary actions to a minimum. The same is true also in the case of the set for disinfecting surgical field, which is justified and fully used up when performing medical procedures in life-threatening conditions. During a resuscitation it is often necessary to apply an endovascular electrode or perform a subclavian vein puncture. Having the complete disinfection set we can take care of the proper preparation of the patient for such procedures in a short time. It is important to save a patient without putting him at any additional risk that after a successful resuscitation may lead to an unwanted contamination. We save the patient and instead “give” him an infection and extended hospital stay. The state of emergency passes, and the patient will require treatment for complications resulting from non-compliance with the basic aseptic principles, the observance of which is certainly facilitated by the Matoset.
M.C. Thank you very much for your time.
‘Wound’ definition
A wound is damage to the skin and sometimes to deeper underlying tissue and even organs as a result of mechanical, thermal or chemical injury. The wounds caused by mechanical injury include: abrasions, cuts, cracks, stab wounds, bite and surgical wounds. The wounds caused by thermal or chemical injury include: all kinds of thermal, chemical, electrical or radiation burns. There are certain types of wounds – chronic (non-healing) wounds, which are caused by other processes – disease processes. Chronic wounds include: pressure ulcers (trophic ulcers), venous ulcers, neuropathic ulcers and ulcers caused by infections and as a result of radiotherapy or neoplastic processes.
Types of wound healing
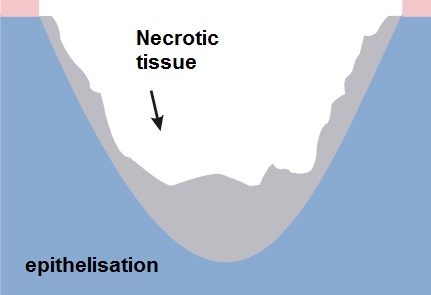
1. Slowly healing wounds – healing by granulation
- significant loss of tissue
- the wound cannot be closed by using physical methods
- long healing time
- the treatment is based on the processes of tissue reconstruction – the defect fills in with granulation tissue, on which epidermis appears and forms a scar
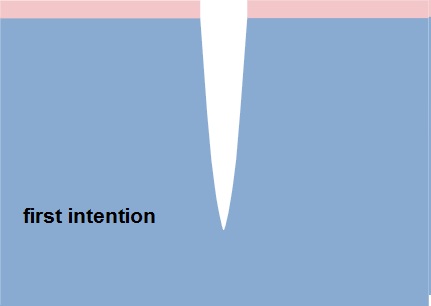
2. Acute wounds – temporary healing by first intention
- surgical or fresh traumatic wounds
- minimum loss of tissue
- edges are joined by seams or using a plaster
Healing phases
There is no one universal dressing that can be used in each case.
Dressings have different functions: cleansing, absorbent and protective, they often complement each other and none of them alone can meet all the needs of the wound passing through the healing stages:
- inflammation phase (exudate)
- granulation and epithelisation phase (growth)
- maturation phase (reconstruction)
Inflammation phase (exudate)
This phase is the body’s response to an injury. Due to circulatory disorders, enlargement and increased permeability of capillaries oedema occurs, accompanied by exudate.
Functions of the dressing in the inflammation phase:
- stemming the bleeding
- facilitating natural debridement
- absorbing excess exudate
- preventing re-infection
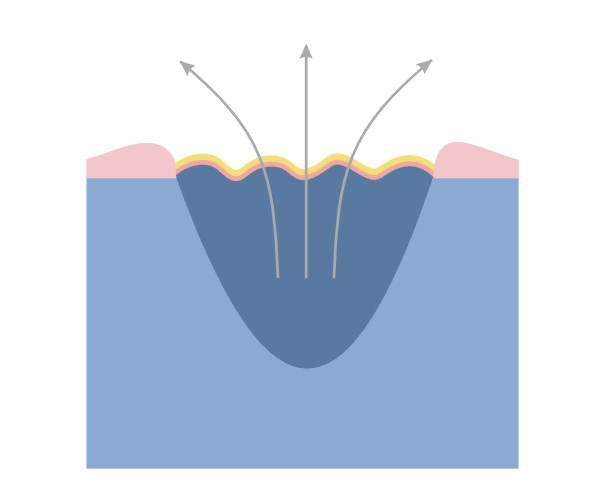
Granulation and epithelising phase (growth)
Granulation – the change from the inflammatory phase into the proliferative phase, which is controlled by macrophages and other cells. Macrophages stimulate fibroblast growth.
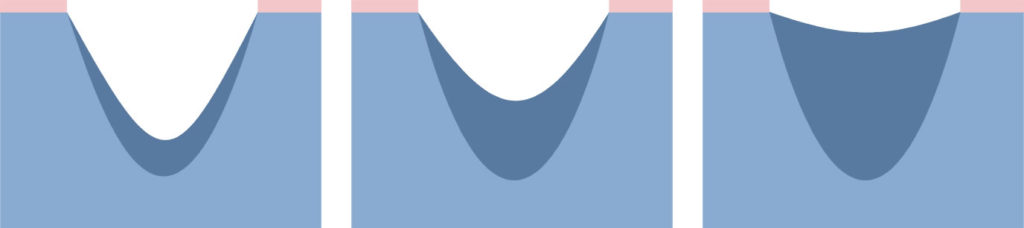
Fibroblasts fill the space that is left after the lost tissue with granulation tissue.
Narrowing of the wound – many fibroblasts is transformed into myofibroblasts. The network of connected myofibroblasts pulls the edges of the wound together (0.6-0.7 mm/day).
Narrowing of the wound makes the scar smaller than the original wound.
Epithelisation – new epidermis, which is needed for the complete closure of the wound. Epidermal cells migrating from the edges of the wound cover the granulation tissue and create new skin.
Functions of the dressing in the growth phase:
Granulation
- maintaining moist environment
- absorbing excess exudate
- protecting against mechanical injury
- preventing re-infection
Epithelisation
- maintain a moist environment
- protecting delicate epidermis during dressing changes
Maturation phase
Maturation – slow reorganisation of microscopic structure of scar tissue; the remodelling results in improving the strength of the scar, its reduction and smoothing.
This stage can last for months or even years.
In the treatment of abnormal scarring are the following items are used:
- topical silicone dressings
- compression bandages or special compression garments
- surgery, corticosteroid therapy, laser and cryosurgery
Functions of the dressing in the maturation phase:
- smoothing the scar
- whitening the scar
- reducing the scar
What is wound exudate?
Wound exudate is a particular fluid called in the past “nature balm” appears in the first stage of wound healing, immediately after an injury.
The exudate contains a variety of ingredients including nutrients for actively metabolising cells:
- very few red blood cells
- up to 6 times more white blood cells than in the blood
- less glucose, but the same amount of minerals as the blood
- proteins – among which there are enzymes important for the wound healing processes; the released enzymes cleanse the wound and remove damaged tissues
In a normally healing wound the amount of exudate decreases with time. In a wound, in which the healing process is disturbed, the amount of exudate is not reduced in time and its management can be a big challenge for dressings.
NOTE: to maintain the best possible conditions for wound healing the optimal amount of wound exudate is needed, namely a so-called moist wound healing environment.
Too much exudate and its absence can slow down the healing process. Therefore, it is important to choose an appropriate dressing to the amount of wound exudate. In wounds dry without exudate the dressing should moisten, and in wounds with too much exudate preferably the dressing should absorb its excess.
NOTE: The change in colour, odour and exudate density may indicate a change in the wound or the appearance of inflammation / infection – it is a signal that the wound should be examined and assessed by a specialist.
Dressing type vs. indication for its use in wounds with various exudate amount
| Dressing type | Level of exudate | ||||
| none | low | medium | high | medium/high | |
| challenge for the dressing | hydrate the wound | maintain a moist environment | absorb the excess of exudate | absorb the excess of exudate | drainage of excess exudate to the secondary dressing |
| hydrogel | √ | √ | |||
| polyurethane film | √ | ||||
| hydrocolloid | √ | √ | |||
| polyurethane foam | √ | √ | |||
| alginate | √ | √ | |||
| resorbable | √ | ||||
Wound treatment models
The traditional wound healing model
Through the centuries chronic wounds were treated using a variety of materials that were to dry the wound.
The traditional wound treatment system based on the use of absorbent dressings made of gauze which:
- ensured the absorption of excess exudate
BUT
- failed to protect the wound against drying out and cooling down, which slowed down the rate of healing
- did not constitute adequate protection against external factors, which could lead to frequent wound infections
- adhered to the wound, which damaged the new tissue and caused pain to the patient during dressing changes
- with limited absorptive capacity compelled to frequent dressing change
Dry wound healing is still the most desirable but for acute wounds healing by first intention.
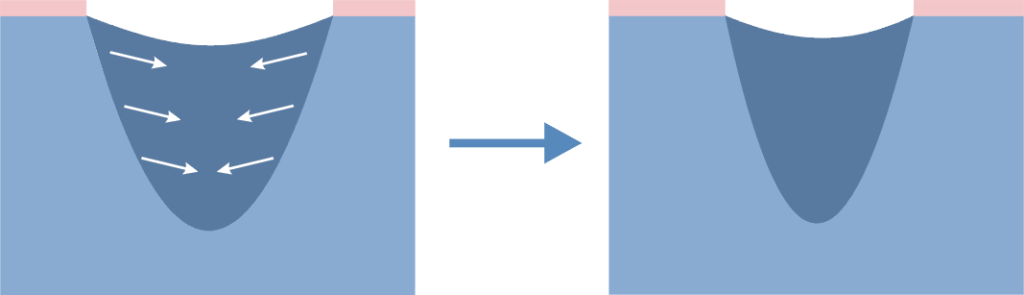
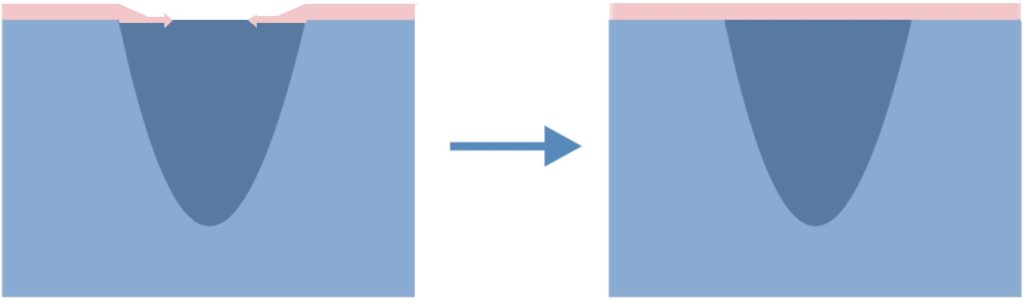
The modern wound healing model
Since the publication of research by George Winter, it became clear that wounds heal much more quickly if the healing process is carried out in humid conditions in which the optimal amount of exudate is maintained on the surface of the wound. In view of the conditions under which the treatment process takes place, the concept was called A MOIST WOUND HEALING.
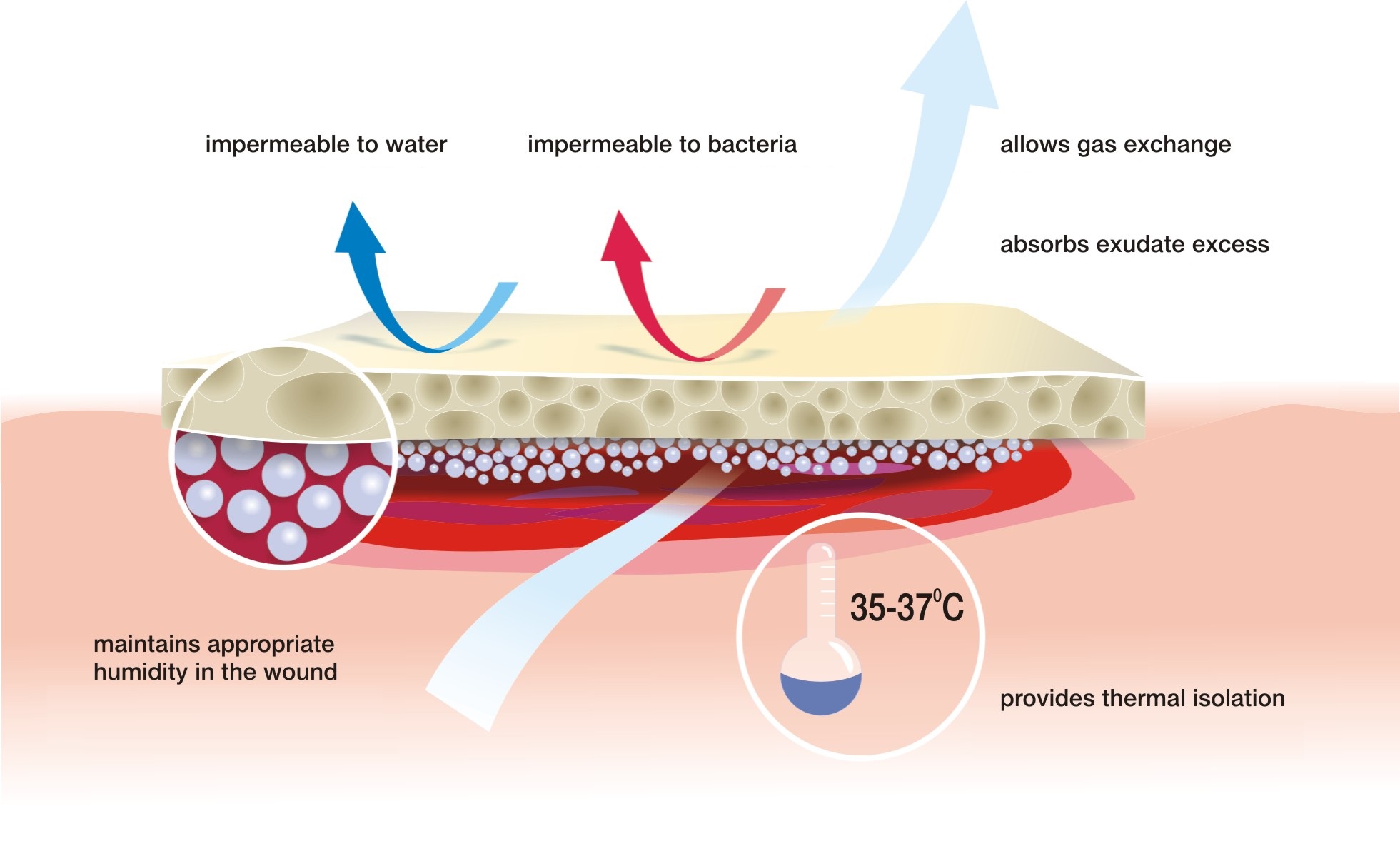
According to this concept, the treatment deals with closing the wound with a special dressing which:
- maintains the required level of moisture on the wound surface to create an optimal healing environment
- initiates autolytic cleansing, which leads to faster debridement and to start the healing process
- thermally isolates the wound which keeps the temperature at a constant level and accelerates the healing process
- provides long-term absorption of excess exudate, reducing the number of dressing changes
- does not adhere to the wound thanks to which dressing change is safe for young tissues and painless for the patient
- is water-resistant and protects the wound against external environment, which minimises the risk of infection
Features of a perfect dressing
Moist wound healing is most appropriate for hard-to-heal wounds but it can be also used for the treatment of usual cuts, abrasions or scratches.
Hanna Szymkiewicz
European Centre for Long-Term Care
A wound is a skin break, which may extend to deeper tissues and organs. The cause of the wound can be internal and external factors associated with physiological disturbances. The breadth and depth of the wound depends on the causative agent, its strength and areas it affected.

Division of wounds due to the causative agent:
>> exogenous factors:
- mechanical (cut, stab, mashed, gunshot wounds)
- thermal (burns, frostbites)
- chemical (chemical burns)
- electrical (burns)
>> endogenous factors
- ulcers (leg ulcers, pressure sores, diabetic foot) – e.g. impaired circulation
Division of wounds due to the healing time:
- sharp – less than 8 weeks
- chronic – more than 8 weeks
Division of wounds due to the way healing:
- acute wounds – cuts, surgical wounds with even edges and in which there is no substantial loss of tissue. Such wounds are closed with sutures, staples or a dressing, and the wound is healed by first intention and lasts about 6-7 days. It is the most preferred way of healing, and is referred to as primary healing.
- chronic wound – wounds where there is a significant loss of tissue and / or infection. In this case, it is not possible to bring the wound edges together. This type of wound healing by granulation (secondary intention) – the inflammatory phase is followed by proliferative phase, in which the tissue loss is filled with granulation tissue. This process is called secondary healing.
Secondary healing
Secondary wound healing concerns chronic wounds – including bedsores, ulcers, and complicated wounds caused by exogenous factors, such as complex surgical wounds. There are three phases in this healing:
- inflammatory phase (purification)
- proliferation (granulation)
- maturation
The inflammatory phase is characterised by an inflammatory reaction and pain. The body is trying to destroy the bacteria that get into the wound after the discontinuation of the skin. Exudate appears. The dead tissues are excreted out or absorbed by the organism. The wound gets covered with blood clot, which protects it from germs.
In the proliferation phase the exudate is reduced, vessels get narrower, and this is followed by granulation – filling the tissue loss and epithelialisation – the wound is covered with new epidermis.
In the maturation phase the rebuilding process of the newly healed wound takes place to get the strength similar to the intact skin.
The process of healing and its duration depends on many different factors: the general condition of the patient: the age, nutritional status and co-existing diseases; the type of the injury, its location, its closure way, its cleanliness and the time that has passes since the injury to its dressing.
Bożena Krymska
Specialist for epidemiological and cardiac nursing – Silesian Centre for Heart Diseases in Zabrze
The quality of medical services means meeting or surpassing the expectations of the patient, the compliance with standards and the degree of realising the benchmarks. According to H. Lenartowicz high-quality health care is one that corresponds to certain criteria, indicating compliance with current professional knowledge and that which, under given circumstances, enables the patients to achieve desired health results. The quality of offered medical services is very important because it concerns the priceless value of life and health of the people making use it.

Although the quality is in fact the satisfaction with well performed medical services, for each party – the performer and the recipient of the service – it means something else.
- For the patient, the quality of medical services depends on the efficient recovery or health improvement after leaving the hospital.
- For employee of the health care facility, the quality is understood as the compatibility of this service with current professional knowledge and achieving health improvement without adverse events.
- For the management of the facility, the quality is to provide services at a sufficiently high level with a correspondingly lower cost.
Any medical procedure performed in a patient comprises several steps:
- preparation of a set,
- performing medical actions,
- disposal of the set, waste management,
- documenting the procedure,
- preparing equipment and reusable instruments for reuse.
Each of these steps requires effort, resources and time. Performing the procedure under various conditions, especially in rapid situations and in emergency rooms, is at high risk of error, which can undoubtedly affect the quality of the procedure, and therefore the quality of the overall medical service.
All of the above steps can be improved by ready-for-use sets adjusted for different procedures and medical treatments. The preparation of a “traditional” set includes the completion of an appropriate amount of equipment, instruments, medicines, and dressing material needed to perform the procedure. However, a ready-for-use set saves the preparation time, especially if the particular procedure is performed urgently. The nurse does not have to wonder how many items to prepare and what exactly is needed. The set provides materials needed to carry out the procedure in terms of their quality and quantity.
The content of the final set forces to perform the procedure in one correct way without omitting certain activities. An example would be the optimum number of six gauze tampons included in the set for bladder catheterisation, which demands to devote enough time to disinfect the area surrounding the urethral meatus, if all the tampons are used. The outer package in form of a rigid blister, often with a few chambers, may serve as a container for liquids or waste material, eliminating the need for additional vessels.
The ready-for-use allow to perform a procedure, opening only one sterile package, which greatly reduces the amount of waste, e.g. many external packaging of: sterile swabs, instruments, gloves, syringes, etc. The sets are completed optimally for a given procedure, which means that any such intervention is carried out using the same amount of equipment and dressing material. In practice, when we complete a set ourselves, there is often a tendency to open more packaging of e.g. dressing material than needed (swabs, cotton balls), just in case, in order not to run out.
The procedure performed using a ready-for-use set quickly becomes standardised, enables to easily monitor the consumption of materials, and thus counting the cost.
It is very easy to clean after the procedure. Everything that has been used is one medical waste. In view of the fact that everything in the set is disposable, the entire material is directed to the waste, without the need to segregate.
It is very simple and accurate to document the performed procedure due to the included self-adhesive labels.
The use of disposable instruments included in the set brings savings, resulting from the elimination of further re-sterilisation. The sterilisation process means additional costs: water, electricity, disinfecting agents, sterilisation packaging, , sterilisation tests, and human effort.
One of the major advantages of the sets is the elimination of adverse events, such as the prevention of infections. Returning to the quality of medical services, the implementation of a program to prevent hospital infections, and systemic efforts to prevent errors in medical procedures is very important to ensure high quality. Reducing the number of infections is an objective indicator of the quality of medical services, and any infection that occurred, and which could have been avoided, is a failure of the institution providing health services. The ready-for-use sets “tailored” to a specific procedure are a perfect tool to prevent such failures. The sets guarantee the sterility of equipment and materials used to perform the procedure. Therefore, the manufacturer takes the responsibility for their sterility, and thus for the quality of the medical device.
Undoubtedly, the application of the sets in practice improves work, gives satisfaction to medical staff, reduces costs, and leads to patient satisfaction. Moreover, better quality of medical care leads to the increased competitiveness of the medical facility in the market.
Literature
- Ciuruś M., Hygiene procedures in health care facilities, Institute for Health Protection, Warsaw 2009.
- Dykowska G., Opolski J., The quality of health care services, self-education package, Warsaw 2001.
- Heczko PB Wójkowska-Mach J. (red.), Hospital infections. Handbook for infection control teams, PZWL, Warsaw 2009.
- Holub, J., Competitive quality strategy on the medical service market, [in:] Nogalski B., Rybicki J. (red.), Modern management of a health care facility, Dom Organizatora, Toruń 2002.
- Lenartowicz H., Quality management in nursing, CEM, Warsaw 1998.
- Maciag A. Kruszewski, K., Topczewska-Tylińska K., Michalak J., The Role of processes, standards and procedures in shaping the quality of health services, Alfa-medica Press, Bielsko-Biala, 2007.
- Piątek, A. Improving the quality of nursing care [in] Ksykiewicz-Dorota A. (red.), Fundamentals of organising nursing care, published by Czelej, Lublin 2004.
Causes
Burns are the result of the action of high temperature, chemical corrosion or current. The most common causes of burns is the heat, which may come from boiling water, steam, hot liquids or semi-liquids like fat or paraffin, as well as burns caused by household appliances.
In electrical burns the main damaging agent is high voltage passing through tissues and heating them. Chemical burns are usually caused by the action of acids or usual alkalis. Regardless of the genesis, burns are specific types of injuries and can cause serious complications for the patient.
Risk group
The risk of burns should be considered in all people, but most of all:
- children at the age 2 to 4 years
- adults working in hazardous conditions (miners, steelworkers, firefighters, welders, etc.)
Symptoms
The main factor determining the type of burn is its depth, by which we distinguish the following types of burns:
- First degree (superficial) – affects only superficial layers of the epidermis. The main symptoms of the damage is vivid red erythema and pain. The wound usually heals without complications and leaves no scars.
- Second degree A (superficial partial thickness) – affects almost the entire layer of the epidermis and superficial dermis. Wounds are usually vivid red, very painful, and are characterised by blisters. 2nd degree burn injury may leave slight discoloration, and sometimes scars.
- Second degree B (deep partial thickness) – the epidermis and deeper dermis layers are destroyed. In this type of injury superficial epidermal and skin necrosis is observed. This type of injury is very painful, blistering free, pale or pink, grey, brick red and even black. Moreover, they can leave negative hypertrophic scars.
- Third degree (full thickness) – extends through entire dermis. The wounds usually are pale brown, brown, pale yellow or red. They leave scars and can lead even to amputation.
- Fourth degree – extends through the entire skin, and into underlying fat, muscles, tendons, bones, joints.
Location
Burns occur in places of body contact with thermal factors.

Typically this affects:
- trunk
- upper limbs
- lower limbs
Where to seek help and advice
First degree burns
can be treated at home, and if there is in the progress in the treatment or complications appear consult your GP
Second and third degree burns
a hydrogel dressing should be applied as soon as possible, e.g. Medisorb G and immediately consult your doctor or contact the emergency station
Fourth degree burns
immediately contact the emergency station or the nearest hospital
Treatment
Depending on the burn degree the treatment is carried out in different ways.
First degree burns – affect only the epithelium. The place that was burned is red, slightly swollen and dry. The victim feels strong burning sensation. Quick application of a hydrogel dressing such Medisorb G allows for quick healing of the wound.
Second degree burns – damage the dermis. It becomes red, and on the surface there are blisters formed that fill with fluid tissue. Second degree burns are very painful. Similarly to the first degree burns rapid response using hydrogel dressings such Medisorb G allows for quick healing. If the burn is extensive, it requires hospitalisation.
Three and four degree burns – affect the tissue located under the skin. Also the connective tissue, blood vessels, muscles, and nerves can get damaged. The skin may take on waxy appearance, whitish or charred colour. The victim may not feel any pain because nerve endings have been destroyed. This type of burns require immediate medical help, sometimes even a skin graft or recovery in the hyperbaric chamber might be needed.
A common complication after recovering from burn wounds are hypertrophic scars and joint contractures. Their long recovery should be carried out using pressotherapy or rehabilitation of scars by means of compression products such as Codopress® combined with silicone dressings Codosil® ADHESIVE.
Prevention
Past statistics show that each year different types of burns affect about 1% of our population. According to these data, the number of Poles affected by various types of burns is up to 400 000 patients per year. Burns are very often associated with the type of activity of patients, as well as with age. Approximately 50-80% of burn victims are mainly children at the age 2 to 4 years.
Prevention of burns should primarily focus on the preparation of the house where the little man will feel safe:
- Never leave a young child alone.
- Avoid placing hot drinks, soups or dishes taken out directly from the oven on a table.
- In homes with young children – especially those crawling ones – there should be no tablecloths – pulling by the tablecloth a child pull down everything what stands on the table.
- Do not leave a turned on iron in the room, where a child is present; a turned off iron must cool down and also be out of reach of children.
- When cooking meals try to do use gas jets at the wall – those being away from your baby; you can use a special shield that prevents a child from touching a hot pot or pull it down.
- Owners of ceramic cooking plates should be aware that a turned off plate does not allow the child to notice the danger, and touching it before it cooled down can result in serious burns.
To sum up – parents should not leave their children unattended!