
Our solutions
No search results
After procedure / surgery
Anna Rogalewska, Patrycja Judycka
Toruńskie Zakłady Materiałów Opatrunkowych SA
Evolving trends in wound dressing
From herbs and leaves, to gauze and bandage, to professional dressings, the practice of wound dressing has been evolving for tens of thousands of years. For over 60 years, Toruńskie Zakłady Materiałów Opatrunkowych (TZMO) has been delivering trend-setting products in wound dressing. Over the years, we have made changes to our range of dressings and the way we make them, but one thing has been constant: we continue to take care to deliver top-quality products that meet the most rigorous safety standards. TZMO’s Matopat-branded medical products have always been a symbol of high quality, innovation and biocompatibility.
Choosing the right dressing: What should patients take into account?
First of all, it’s the kind of wound, as different wounds heal differently. You will need a different dressing for a surgical wound, or incision (such wounds must be dressed precisely, in a sterile manner, by qualified medical personnel in a suitable place), a different one for a new post-injury wound and a yet different one for a difficult-to-heal wound with substantial tissue loss. Once you have identified the kind of wound you’re dealing with, you need a professional dressing that will not only reduce the risk of infection and offer optimal healing time and effectiveness, but also help the patient feel more comfortable. There has been a noticeable trend in the use of professional wound dressings: in the past, they were used only by medical professionals in hospitals, but now they are making their way to pharmacies. As a result, professional wound dressings can today be used by patients at home.
The properties of professional wound dressings
For a small cut or chafe, a clean and comfortable sticking plaster will do the job. Apply it to the affected area and leave it for a scab to form and the wound to heal. However, in the case of more serious wounds, such as surgical wounds, it is advisable to use professional dressings such as those used in hospitals. Professional surgical dressings are sterile, absorptive and flexible, and designed so that the adhesive can keep the dressing tight on the affected area, preventing dirt or other unwanted matter from penetrating the wound. At the same time, the absorption material should be sufficiently protected to prevent direct contact of the dressing with the surface of the wound or with the surgical sutures. Professional dressings are also air-permeable to allow the skin to “breathe”.
 Examples of professional dressings for surgical wounds include Fixopore S and Fixopore F. The former is made of flexible, nonwoven fabric that easily fits in even hard-to-access areas of the patient’s body and will not limit the patient’s movement. A nonwoven fabric dressing is the basic type of dressing used by hospitals for surgical wounds. This dressing has a special, smooth layer of absorption material that will not get stuck on the wound or suture, thus allowing for safe and painless dressing changes without the risk of damage to the absorption material. The adhesive on the dressing is hypoallergenic. The other of the two products, Fixopore F, is made of ultra-thin polyurethane film that keeps moisture away from the wound. This helps patients to go about their regular daily activities without having to change their dressings frequently and without the risk of infecting the wound. The benefits of modern wound dressings can be enjoyed fully if the dressings are used in accordance with the user’s instructions.
Examples of professional dressings for surgical wounds include Fixopore S and Fixopore F. The former is made of flexible, nonwoven fabric that easily fits in even hard-to-access areas of the patient’s body and will not limit the patient’s movement. A nonwoven fabric dressing is the basic type of dressing used by hospitals for surgical wounds. This dressing has a special, smooth layer of absorption material that will not get stuck on the wound or suture, thus allowing for safe and painless dressing changes without the risk of damage to the absorption material. The adhesive on the dressing is hypoallergenic. The other of the two products, Fixopore F, is made of ultra-thin polyurethane film that keeps moisture away from the wound. This helps patients to go about their regular daily activities without having to change their dressings frequently and without the risk of infecting the wound. The benefits of modern wound dressings can be enjoyed fully if the dressings are used in accordance with the user’s instructions.
Educating patients
A pharmacist’s role is not only to help patients choose the right dressing, but also to educate them about the need for taking proper care of their wounds. Wound cleaning and correct dressing changes are essential and, apart from the choice of dressing, will help the wound to heal quickly and without complications. A general rule in professional wound healing is that dressing changes should be as rare as possible, following the recommended dressing use time, and as frequent as possible, depending on the appearance of the wound and the condition of the dressing.
For more information about professional dressings for different wound types, please visit: en.matopat-global.com
Yearly about 1% of our population gets burned. The number of Poles affected by burn injuries reaches even 400,000 patients a year. Mostly 50-80% of the burned are children in the 2-4-year-old age group.
Burns can be divided by depth:

- 1st degree – a superficial burn. Only the surface layers of the skin are affected. The symptoms include redness (erythema) and painfulness. The wound usually heals without any complications and scars.
- 2nd A degree – extends into superficial (papillary) dermis. Those wounds are usually very red with clear blisters and are extremely painful. After 2nd A injuries there might appear small discolorations or even scars.
- 2nd B degree – extends into deep (reticular) dermis. In those type of burns superficial epidermal and dermal necrosis might appear. Those wounds are very painful, without blisters, pale or pinkish, grey, bricky or even black. Moreover, they may leave nasty hypertrophied scars.
- 3rd degree – extends through entire dermis. These wounds are usually russet, brown, pale yellow or red.
- 4th degree – extends through skin, subcutaneous tissue and into underlying muscles, tendons, bones, joints.
In the 3rd and 4th degree burns the skin reproductive layer is impaired or completely damaged.
Complications of burns
Quite a frequent complication of burns are hypertrophied scars and joint contractures. The hypertrophied scars appear, among other things, as a result of the increase in blood flow, fibroblast development and collagen deposition as well as of chronic oedema. In all those cases, when strong redness of the scar does not disappear up to two months, and the scar gets thicker and thicker, a keloid scar is very likely to develop. Keloids have a lumpy structure, which is a result of increased metabolism. Their growth is stimulated by microphages and fibroblasts, evoking an overgrowth of collagen fibres. Those complications are inconvenient because they delimit the functioning of the motor apparatus and at the same time they blemish the affected person.
Prophylactically appropriate positioning of the body and joint immobilisation by means of splints or orthopaedic devices is practised. It has also been proven that the application of constant pressure, increasing the capillary pressure of vessels i.e. about 25-30 mmHg, has a beneficial influence on scar formation, and prevents the overgrowth to a large extent. A long-lasting pressure causes an oxygen deficiency in tissues, a deceleration in metabolism and a fibroblast reduction. An increase in the activity of a collagen-decomposing enzyme (collagenase) results in a visible scar reduction.
The pressure method in supporting the post-burn scar treatment has been worldwide known for many years, and it is also commonly used in Poland. The pressotherapy is found to be the most effective method, though there are many alternative ones such as laser therapy, kriotherapy etc.
Apart from negative health effects, quite often the keloids are also harmful to patients’ mental state, resulting sometimes in social exclusion. In modern techniques, and medical procedures it is clearly stated that an effective post-burn rehabilitation needs to be designed in such a way to reduce the keloid formation. An important element of modern treatment support techniques is the application of compression combined with the activity of silicone dressings like e.g. CodosilTM ADHESIVE.
Mechanism of post-burn scar formation
Every wound has the possibility of self-healing. Superficial wounds, in which the topmost layer of the skin (the epidermis) is scraped off, heal without leaving any scars. At the beginning of the healing process the wound is cleansed, so there appear a lot of macrophages and histiocytes. The neoformation of capillaries is evoked, facilitating the appearance of multipotent cells – lymphocytes, which have the ability to turn into fibroblasts. A fibroblast is a type of a cell that synthesises the macromolecules building connective tissue. This cell synthesises tropocollagen, which by polymerisation creates collagen fibres. As those fibres get created, the involution of capillaries takes place, the activity of fibroblasts is lost, and the reepithalisation process is initiated.
In burns, when the epidermis, the papillary layer and the reticular layer get damaged, a stronger hyperplasia of vessels is observed. The widening of vessels, and the appearance of anastomoses causes blood to stop in the healing place, and provides a good access to nutrients; a lot of highly active fibroblasts appear as a result of the production of a great number of collagen fibres.
The reconstruction along with the scar formation takes place at the newly created fibroblasts’ expense, where gradually myofibroblasts – responsible for contractility – get distinguished, while mastocytes take care of the progressive maturation of the scar. Biochemical tests of a scarring process show that there is an increased collagen synthesis in comparison with a normal healing process, and there are also qualitative disorders connected with the increase in the number of mucopolysaccharide matrices, and the decrease in the number of lipids (mainly linolic acid) in the scar. It seems that the reason for this lies in the reduced amount of collagenase (a collagen-decomposing enzyme), resulting from the increase of 1 – antitrypsin and 2 – mucoprotein globulins. Those effects occur probably along with a toxic mitochondrial activity in the damaged cells. This activity takes place in burns from the first moment up to the 10th day of the healing process, when it is possible to notice that those symptoms stop, and a gradual comeback to a normal state, or also an objective steady growth takes place up to the 14th and after the 21st day, if any scarring complications appear.
Moreover, also the effect of the adrenal gland on scar fibroblasts, and their uncontested influence on scarring processes has been recognised. This is the base to examine possible mutual correlations between the prevalence of scarring complications and endocrinological changes in children. Obviously such a correlation takes place during a burn shock, and its further development is not known. Topical scar complications developing after a burn can be either of an aesthetic or of a functional type, or of both types simultaneously. From a histopathological point of view the cicatrical changes are of a hypertrophic, a contractile or a keloid type. Popularly it is said that this happens in 50% of burn cases; however, the factors indicating those changes has not been determined yet. Their impact on the early estimation of an actual scar development possibility is also not known. Especially when it goes about keloids – they are likely to develop even in 80% of places vulnerable to stretching or tension.
Pressotherapy – an effective therapeutic method for post-burn scars
An elastic pressotherapy as a preventive and therapeutic method started to evaluate in the 70s, and turned out to be very effective in supporting the treatment of post-burn complications. This method involves using hypercompression (or just compression) to give constant pressure on keloids. This pressure on the scar gives an ischemic effect, which makes afferent vessels smaller, which results in the reduction of vessel embryos. On one hand, the scar will be supplied with less blood if we reduce the number of blood vessels, but on the other hand, depending on the diameter of the vessel embryos, the blood flow will be increased, and there will be no stasis, which will further influence the reduction of produced collagen fibres, and prevent the wound area from shrinking.
A correctly applied pressotherapy involves the use of strong pressure on the wound after finished epithelisation by means of different types of bandages made of natural latex. Such products are produced of latex threads covered with synthetic fibres.
Their application on the scar and the stable pressure they give can change and improve the content and the quality of various tissue elements. This change in the tissue components results in the qualitative improvement, weakening and decreasing the size of the scar, and at the same time due to the accompanying ischemia, the characteristic red colour of the scar is fading.
General rules for the use of pressotherapy:
- the pressure should be applied as soon as possible (from the moment of wound re-epithelisation, during the next 2-3 years – this is the estimated time for scar development), more or less 1 or 1,5 year;
- constant uninterrupted and long-lasting application of pressure on cicatrical places through an individual adjustment of special compression garments with compression level from 20-25 up to 50 mm Hg/cm2.
To reach the best results it is necessary to observe and control the entire process of the compression rehabilitation, and to change the compression garment periodically since the knitted fabric loses its elasticity, or the patient’s size might change as well.
The time of the compression therapy is varied – optimally up to 2 years. If any topical complications appear such as skin irritation, intertrigo, skin breaks or patient’s psychical inconvenience – the pressotherapy should be temporarily interrupted and then repeated, trying to eliminate those symptoms. [1]
Compression levels in pressotherapy
Compression clothing is characterised by a precisely defined pressure level exerted on the patient’s body. The pressure is expressed in a unit – millimetre of mercury (mmHg). The efficiency depends on the size of the garment, which is to be individually adjusted to a given person after taking precise measures of the patient’s body. The effectiveness of the therapy is also affected by the choice of an appropriate compression level, which depends on the disorder type and its severity. It is highly important to choose the right compression level of a compression product, for too little pressure will bring no effect, and too big pressure can cause many undesirable side effects. The complications may start from very simple ones such as chafes, abrasions or maceration, up to more serious ones such as serous blisters or decubitus ulcers. Those and other side effects resulting from a wrongly chosen compression level, quite often make the patient break the therapy.
The most popularly used compression level classification is the one used in Germany, Switzerland and Italy. In all types of classifications class 1 means the lightest compression, and class 4 the strongest compression. The values express compression given by a product at the ankle joint high. It is important to maintain a compression gradation given on the limb at the entire length of the product. In this case usually there is a rule applied to use 100% compression of the given class (from 1 to 4) at the ankle high (distal part of the product), up to 40% of the compression in the closer (proximal) part.
Producers use different classifications of compression; however, the one specified by the European Standardisation Commission distinguishes the following ones:
- class 1 – light compression (18-21 mmHg),
- class 2 – medium compression (23-32 mmHg),
- class 3 – strong compression (34-46 mmHg),
- class 4 – very strong compression (over 49 mmHg).
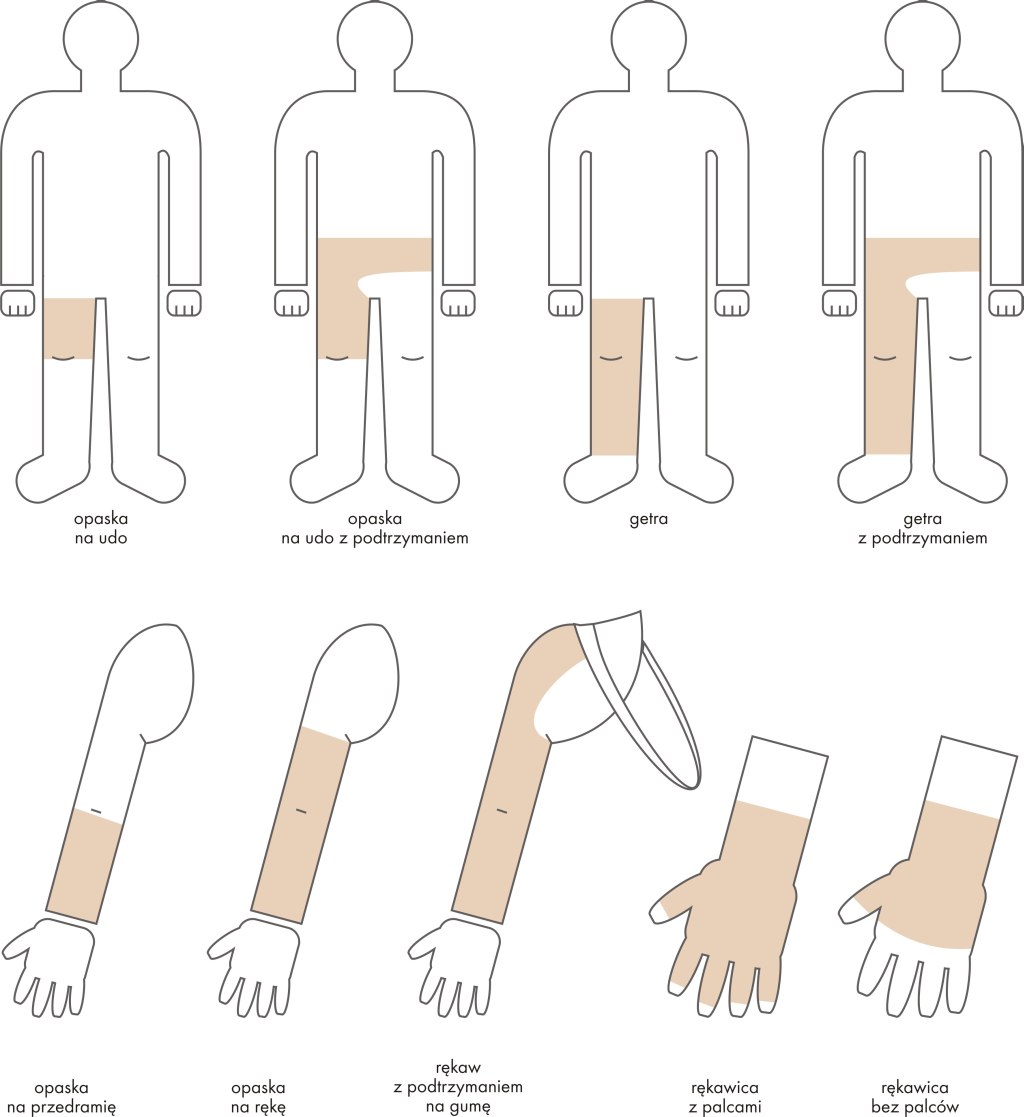
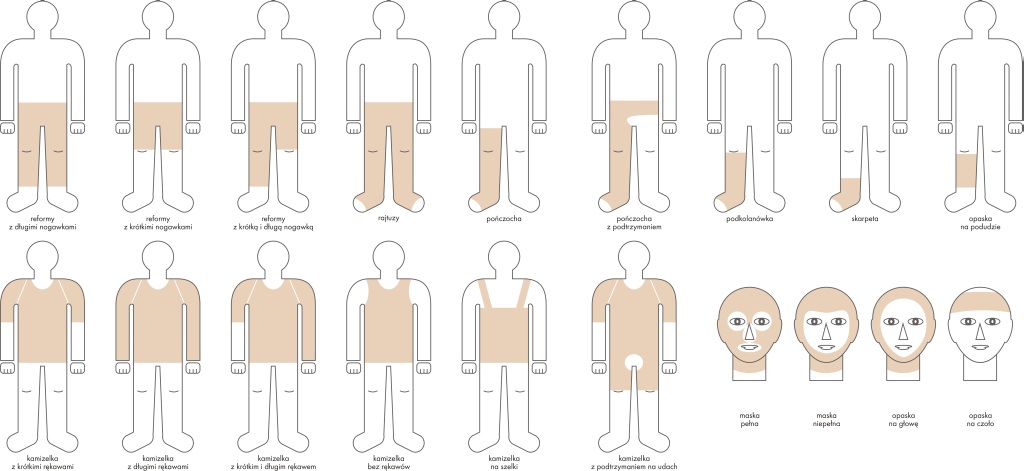
Efficient therapy with the application of compression garments Codopress®
The success of the therapy highly depends on appropriately chosen compression clothing. Compression garments Codopress® produced in Łódź (Poland) by Tricomed SA are used for supporting the treatment of post-burn scars and in prophylactic rehabilitation of burns. Up till now over 20 thousand products Codopress® have been prepared, successively developing the product range, and improving the construction. The garment is produced of a highly elastic breathable knitted fabric of medical quality, composed of a polyurethane and polyamide yarn. This combination enables to obtain required parameters, and at the same time to provide high comfort for the user.
The manufacturing process makes it possible to produce the garment for every body part according to the compression class recommended by a doctor. The 1st class compression (18-21 mmHg) is the one most frequently used. It is remarkable that all compression products Codopress® are manufactured so that all seams are aside from all scars. Thanks to this the value of the therapeutic pressure is not changed in any way in this place.
The process of compression garment preparation:
- Get a referral from a specialist.
- Make an appointment with a person taking measures of the limb or other body parts.
- Once the garment is sewn it needs to be tried on to make sure that it fits perfectly.
- The patient is trained how to use and clean the product.
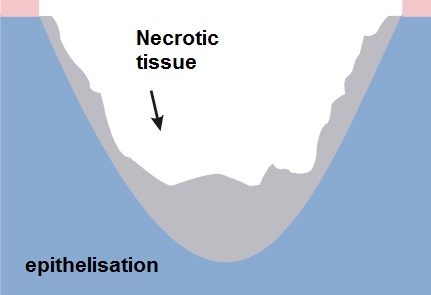
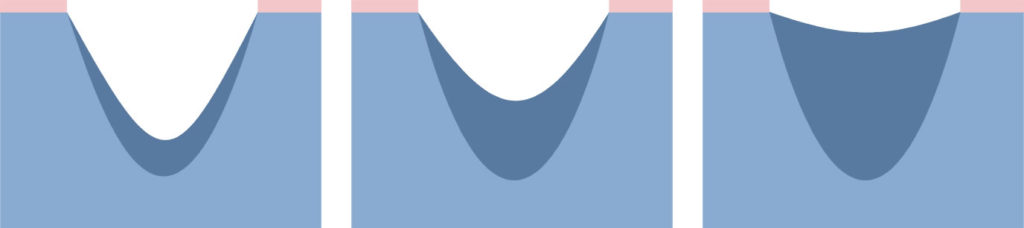
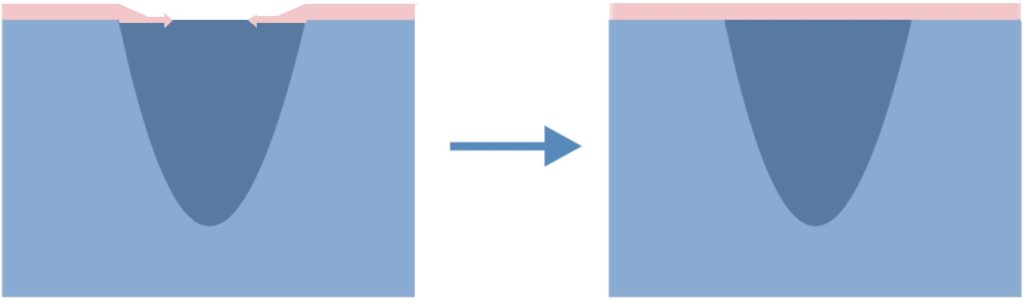
All compression garments should be worn permanently from 6 to 24 months after the wound healing process is finished, till visible rehabilitation effects appear (flattening, fading and softening). The entire therapy usually requires a few changes of the compression garments, along with the use up of the garment and the change of patient’s body size. It is important to remember to use the products only when the post-burn wound is fully healed – see pictures below:


Individually prepared Codopress® products:
- give appropriate compression on the scar,
- can be used with other types of therapy,
- cause no allergic reactions or skin irritations,
- release itching,
- prevent from joint contractures.
Clinical trials
In specialised burn healing centres in Siemianowice (Poland) and Polanica Zdrój (Poland) – leading centres healing heavy burns – a wide range of patients were clinically examined. They tested the effectiveness of Codopress® products in the rehabilitation of post-scar burns.
Clinics testing the Codopress® clothing included the Burn Treatment Ward of the Municipal Hospital No. 2 in Siemianowice Śląskie ran by S. Sakiel, MD, and the Plastic Surgery Hospital in Polanica Zdrój under the supervision of K. Kobus, PhD, Dr h. c. What is more in the National Medicines Institute under the direction of W. Zalewski, PD tests were carried out as for the irritating effect on the skin of the knitted textile used in the production of Codopress® products.
Materials and methods
Within 2 years compression products produced by Tricomed SA were tested in 40 patients at the age of 2 to 59 years old with the average burn area of 26%, and deep burns at the entire skin depth with the average area of 9%.
The patients were divided into two groups:
- in the first group (20 patients) the compression products were applied right after the wound was healed,
- in the second group (20 patients) the Codopress® products were applied after about 3 months after the wound was healed.
The evaluation concerned the face, the neck, the chest, the upper and lower limbs. Overall in the first group 24 places and in the second group 30 places were observed.
 The tested products were evaluated as for their usefulness in supporting the treatment of hypertrophied scars and keloids in 26 patients aged 3 to 58 years. Most of the hypertrophied scars and keloids were caused by hot fluids or fire. The entire healing period for a burn wound, starting from the application of the compression products, took a month up to 4 years. Before the application of pressotherapy, massages were applied. Body parts that were most often tested as for the usefulness of the compression products included: the knee and elbow joint, the buttocks, the hips, the shoulders, the chest, the upper and lower limbs.
The tested products were evaluated as for their usefulness in supporting the treatment of hypertrophied scars and keloids in 26 patients aged 3 to 58 years. Most of the hypertrophied scars and keloids were caused by hot fluids or fire. The entire healing period for a burn wound, starting from the application of the compression products, took a month up to 4 years. Before the application of pressotherapy, massages were applied. Body parts that were most often tested as for the usefulness of the compression products included: the knee and elbow joint, the buttocks, the hips, the shoulders, the chest, the upper and lower limbs.
Test results
The results of the carried out tests indicated that in hypertrophied scars and keloids treated with the compression products sweeping changes were noticed. The itch observed in 8 cases retreated after 3 weeks. The colour of fresh scars changed from bloody pale into flesh-like in 17 patients after 4 weeks. The height of the scar was reduced from average 4 mm at the beginning (measured from the healthy skin) up to 0-2 mm. The best results were observed in fresh scars, which were 4 weeks old. In the case of older scars those effects were visible after a longer period of time.
There were no allergic reactions noted. Washing by means of commonly available washing agents and an all-day-long utilisation did not affect the elasticity of the tested products. The best therapeutic results were observed on tights, lower legs and forearms. The patients had no objection to wearing the compression garments. All in all compression products Codopress® undoubtedly contribute to faster rehabilitation of patients with after-burn deformations.
The summary of test results
While wearing Codopress® products for a few months the following conclusions were made:
- the scars were getting flatter,
- the extremely red colour was gradually fading,
- no allergic reactions to the material in Codopress® products were observed,
- in the same patients comparing not pressed scar places with the ones pressed by means of Codopress® clothing there were visible differences in form of hypertrophies and hard scars in the not pressed places,
- the application of the compression clothing just after the wound was healed brought better effects than in patients who used the products after hypertrophied scars appeared. [2]

Conclusions
- The tested products Codopress® are very useful in the prophylaxis and rehabilitation of hypertrophied scars.
- Compression garments need to be tailored according to the measured body dimensions of the wearer in order to provide high efficiency.
- An early application (just after the wound is healed) of tailor-made compression products guarantees the best efficiency of the scar rehabilitation.
- Constant wear of the clothing (13 hours a day) 1 to 2 years changed only if it is worn up or the patient’s size has changed:
- prevents the development of hypertrophied scars,
- causes the reduction and, in most cases, the regression of keloids,
- improves the final aesthetic look.
- Pressotherapy enables to continue physical rehabilitation and does not constrain the patient’s activity after the burn.
- The knitted fabric used in Codopress® products causes no irritating reactions.
[separator]
Associable therapy Codopress® + Codosil™ ADHESIVE
Silicone dressings adjunctive to scar treatment by means of pressotherapy have gained in popularity in the past 10 years. Their application decreases the growth of small blood vessels in a scar, and as a result the scar gets more elastic and flatter.

Many specialists recommend the associable therapy, combining a few methods individually adjusted to a given patient. One of them is compression therapy joined with dressings meant for scar rehabiitation. The dressing used for this type of combined therapy is CodosilTM ADHESIVE.
CodosilTM ADHESIVE is a soft multi-layer product designed for the rehabilitation of hypertrophied scars and keloids. Adhesive silicone layer is in the direct contact with the scar surface. The outer side of the dressing is secured with an anti-adhesive protection layer.
- releases the itching and pain,
- does not present irritating and sensitising properties,
- is susceptible to folding,
- reveals sticky properties which makes it possible to stick to the skin’s surface repeatedly,
- is meant for multiple use,
- is easy to store and apply.
 The silicone dressing can be applied as a preventive agent when the wound is fully closed (8-10th day) or when first symptoms of a hypertrophied scar appear. Early application of the dressing increases the chance of proper scar rehabilitation.
The silicone dressing can be applied as a preventive agent when the wound is fully closed (8-10th day) or when first symptoms of a hypertrophied scar appear. Early application of the dressing increases the chance of proper scar rehabilitation.
The dressing is used only on skin that is not broken, remembering to make the dressing 1 cm bigger than the scar size. Prophylactically it should be worn 12 hours a day. In patients using the compression products Codopress® along with the silicone dressing CodosilTM ADHESIVE there were visible therapeutic effects observed: flattening, fading and softening of the scar. Moreover, the motor activity is improved and the risk of contractures is limited.
CodosilTM ADHESIVE is recommended to be used:
- in rehabilitation of hypertrophied scars and keloids,
- as prophylaxis in people with hypertrophied scar and keloid tendencies,
- in cosmetology for the rehabilitation of scars after aesthetic surgery.
Literature:
[1] Babiana Mossakowska, PhD, Professor, Presoterapia u dzieci (Pressotherapy in children).
[2] A. Nawrocki, doc., PhD, and others, Ocena kliniczna – Opracowanie technologii i ocena artykułów medycznych do zastosowania w chirurgii plastycznej (Clinical evaluation – The compilation of technologies and the evaluation of medical products to be applied in plastic surgery).
All Codopress® products are individually prepared after taking measures. To make an appointment and get more information please contact us export@tzmo.com.pl.
‘Wound’ definition
A wound is damage to the skin and sometimes to deeper underlying tissue and even organs as a result of mechanical, thermal or chemical injury. The wounds caused by mechanical injury include: abrasions, cuts, cracks, stab wounds, bite and surgical wounds. The wounds caused by thermal or chemical injury include: all kinds of thermal, chemical, electrical or radiation burns. There are certain types of wounds – chronic (non-healing) wounds, which are caused by other processes – disease processes. Chronic wounds include: pressure ulcers (trophic ulcers), venous ulcers, neuropathic ulcers and ulcers caused by infections and as a result of radiotherapy or neoplastic processes.
Types of wound healing
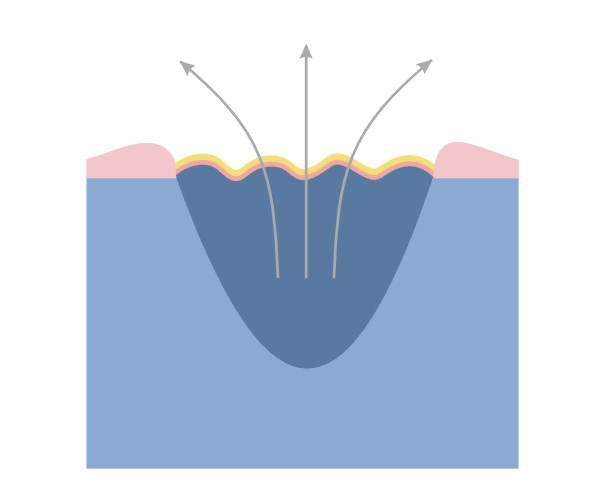
1. Slowly healing wounds – healing by granulation
- significant loss of tissue
- the wound cannot be closed by using physical methods
- long healing time
- the treatment is based on the processes of tissue reconstruction – the defect fills in with granulation tissue, on which epidermis appears and forms a scar
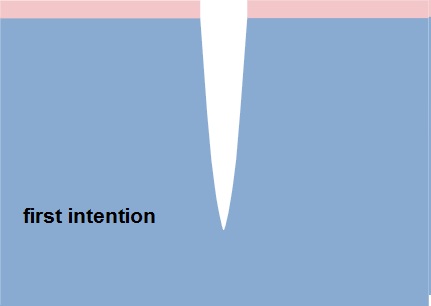
2. Acute wounds – temporary healing by first intention
- surgical or fresh traumatic wounds
- minimum loss of tissue
- edges are joined by seams or using a plaster
Healing phases
There is no one universal dressing that can be used in each case.
Dressings have different functions: cleansing, absorbent and protective, they often complement each other and none of them alone can meet all the needs of the wound passing through the healing stages:
- inflammation phase (exudate)
- granulation and epithelisation phase (growth)
- maturation phase (reconstruction)
Inflammation phase (exudate)
This phase is the body’s response to an injury. Due to circulatory disorders, enlargement and increased permeability of capillaries oedema occurs, accompanied by exudate.
Functions of the dressing in the inflammation phase:
- stemming the bleeding
- facilitating natural debridement
- absorbing excess exudate
- preventing re-infection
Granulation and epithelising phase (growth)
Granulation – the change from the inflammatory phase into the proliferative phase, which is controlled by macrophages and other cells. Macrophages stimulate fibroblast growth.
Fibroblasts fill the space that is left after the lost tissue with granulation tissue.
Narrowing of the wound – many fibroblasts is transformed into myofibroblasts. The network of connected myofibroblasts pulls the edges of the wound together (0.6-0.7 mm/day).
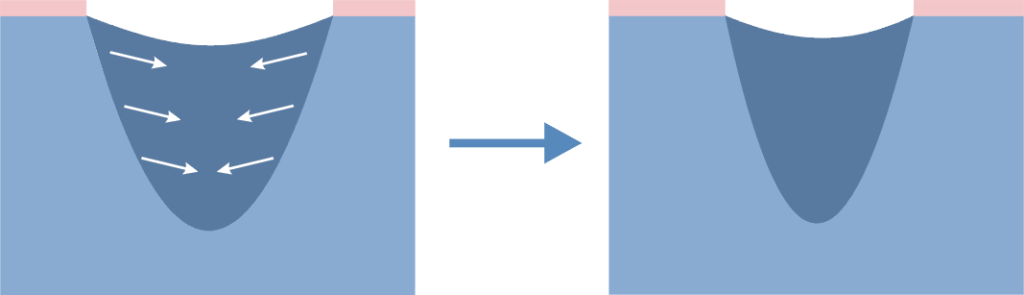
Narrowing of the wound makes the scar smaller than the original wound.
Epithelisation – new epidermis, which is needed for the complete closure of the wound. Epidermal cells migrating from the edges of the wound cover the granulation tissue and create new skin.
Functions of the dressing in the growth phase:
Granulation
- maintaining moist environment
- absorbing excess exudate
- protecting against mechanical injury
- preventing re-infection
Epithelisation
- maintain a moist environment
- protecting delicate epidermis during dressing changes
Maturation phase
Maturation – slow reorganisation of microscopic structure of scar tissue; the remodelling results in improving the strength of the scar, its reduction and smoothing.
This stage can last for months or even years.
In the treatment of abnormal scarring are the following items are used:
- topical silicone dressings
- compression bandages or special compression garments
- surgery, corticosteroid therapy, laser and cryosurgery
Functions of the dressing in the maturation phase:
- smoothing the scar
- whitening the scar
- reducing the scar
What is wound exudate?
Wound exudate is a particular fluid called in the past “nature balm” appears in the first stage of wound healing, immediately after an injury.
The exudate contains a variety of ingredients including nutrients for actively metabolising cells:
- very few red blood cells
- up to 6 times more white blood cells than in the blood
- less glucose, but the same amount of minerals as the blood
- proteins – among which there are enzymes important for the wound healing processes; the released enzymes cleanse the wound and remove damaged tissues
In a normally healing wound the amount of exudate decreases with time. In a wound, in which the healing process is disturbed, the amount of exudate is not reduced in time and its management can be a big challenge for dressings.
NOTE: to maintain the best possible conditions for wound healing the optimal amount of wound exudate is needed, namely a so-called moist wound healing environment.
Too much exudate and its absence can slow down the healing process. Therefore, it is important to choose an appropriate dressing to the amount of wound exudate. In wounds dry without exudate the dressing should moisten, and in wounds with too much exudate preferably the dressing should absorb its excess.
NOTE: The change in colour, odour and exudate density may indicate a change in the wound or the appearance of inflammation / infection – it is a signal that the wound should be examined and assessed by a specialist.
Dressing type vs. indication for its use in wounds with various exudate amount
| Dressing type | Level of exudate | ||||
| none | low | medium | high | medium/high | |
| challenge for the dressing | hydrate the wound | maintain a moist environment | absorb the excess of exudate | absorb the excess of exudate | drainage of excess exudate to the secondary dressing |
| hydrogel | √ | √ | |||
| polyurethane film | √ | ||||
| hydrocolloid | √ | √ | |||
| polyurethane foam | √ | √ | |||
| alginate | √ | √ | |||
| resorbable | √ | ||||
Wound treatment models
The traditional wound healing model
Through the centuries chronic wounds were treated using a variety of materials that were to dry the wound.
The traditional wound treatment system based on the use of absorbent dressings made of gauze which:
- ensured the absorption of excess exudate
BUT
- failed to protect the wound against drying out and cooling down, which slowed down the rate of healing
- did not constitute adequate protection against external factors, which could lead to frequent wound infections
- adhered to the wound, which damaged the new tissue and caused pain to the patient during dressing changes
- with limited absorptive capacity compelled to frequent dressing change
Dry wound healing is still the most desirable but for acute wounds healing by first intention.
The modern wound healing model
Since the publication of research by George Winter, it became clear that wounds heal much more quickly if the healing process is carried out in humid conditions in which the optimal amount of exudate is maintained on the surface of the wound. In view of the conditions under which the treatment process takes place, the concept was called A MOIST WOUND HEALING.
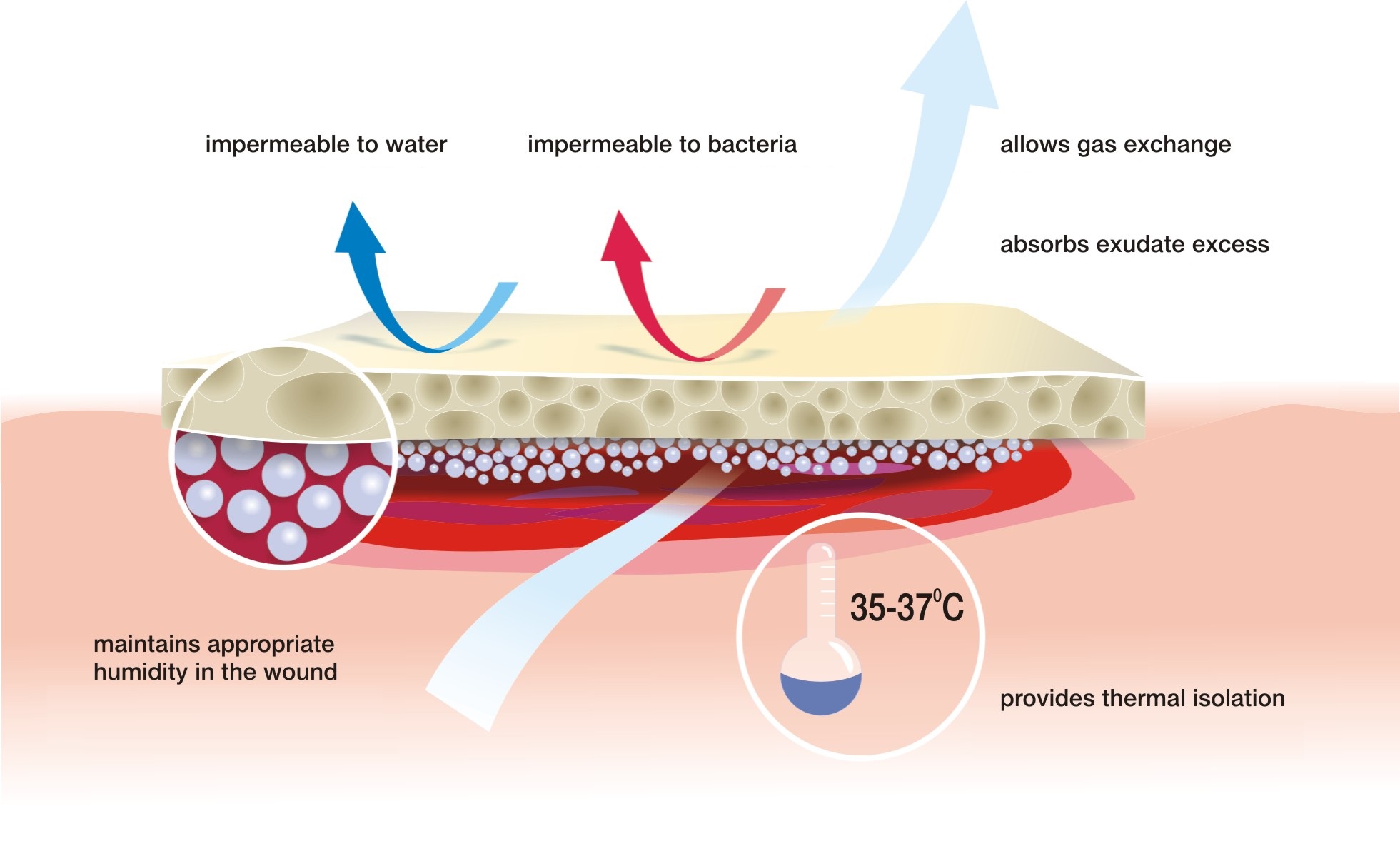
According to this concept, the treatment deals with closing the wound with a special dressing which:
- maintains the required level of moisture on the wound surface to create an optimal healing environment
- initiates autolytic cleansing, which leads to faster debridement and to start the healing process
- thermally isolates the wound which keeps the temperature at a constant level and accelerates the healing process
- provides long-term absorption of excess exudate, reducing the number of dressing changes
- does not adhere to the wound thanks to which dressing change is safe for young tissues and painless for the patient
- is water-resistant and protects the wound against external environment, which minimises the risk of infection
Features of a perfect dressing
Moist wound healing is most appropriate for hard-to-heal wounds but it can be also used for the treatment of usual cuts, abrasions or scratches.
Hanna Szymkiewicz
European Centre for Long-Term Care
A wound is a skin break, which may extend to deeper tissues and organs. The cause of the wound can be internal and external factors associated with physiological disturbances. The breadth and depth of the wound depends on the causative agent, its strength and areas it affected.

Division of wounds due to the causative agent:
>> exogenous factors:
- mechanical (cut, stab, mashed, gunshot wounds)
- thermal (burns, frostbites)
- chemical (chemical burns)
- electrical (burns)
>> endogenous factors
- ulcers (leg ulcers, pressure sores, diabetic foot) – e.g. impaired circulation
Division of wounds due to the healing time:
- sharp – less than 8 weeks
- chronic – more than 8 weeks
Division of wounds due to the way healing:
- acute wounds – cuts, surgical wounds with even edges and in which there is no substantial loss of tissue. Such wounds are closed with sutures, staples or a dressing, and the wound is healed by first intention and lasts about 6-7 days. It is the most preferred way of healing, and is referred to as primary healing.
- chronic wound – wounds where there is a significant loss of tissue and / or infection. In this case, it is not possible to bring the wound edges together. This type of wound healing by granulation (secondary intention) – the inflammatory phase is followed by proliferative phase, in which the tissue loss is filled with granulation tissue. This process is called secondary healing.
Secondary healing
Secondary wound healing concerns chronic wounds – including bedsores, ulcers, and complicated wounds caused by exogenous factors, such as complex surgical wounds. There are three phases in this healing:
- inflammatory phase (purification)
- proliferation (granulation)
- maturation
The inflammatory phase is characterised by an inflammatory reaction and pain. The body is trying to destroy the bacteria that get into the wound after the discontinuation of the skin. Exudate appears. The dead tissues are excreted out or absorbed by the organism. The wound gets covered with blood clot, which protects it from germs.
In the proliferation phase the exudate is reduced, vessels get narrower, and this is followed by granulation – filling the tissue loss and epithelialisation – the wound is covered with new epidermis.
In the maturation phase the rebuilding process of the newly healed wound takes place to get the strength similar to the intact skin.
The process of healing and its duration depends on many different factors: the general condition of the patient: the age, nutritional status and co-existing diseases; the type of the injury, its location, its closure way, its cleanliness and the time that has passes since the injury to its dressing.
Causes
Burns are the result of the action of high temperature, chemical corrosion or current. The most common causes of burns is the heat, which may come from boiling water, steam, hot liquids or semi-liquids like fat or paraffin, as well as burns caused by household appliances.
In electrical burns the main damaging agent is high voltage passing through tissues and heating them. Chemical burns are usually caused by the action of acids or usual alkalis. Regardless of the genesis, burns are specific types of injuries and can cause serious complications for the patient.
Risk group
The risk of burns should be considered in all people, but most of all:
- children at the age 2 to 4 years
- adults working in hazardous conditions (miners, steelworkers, firefighters, welders, etc.)
Symptoms
The main factor determining the type of burn is its depth, by which we distinguish the following types of burns:
- First degree (superficial) – affects only superficial layers of the epidermis. The main symptoms of the damage is vivid red erythema and pain. The wound usually heals without complications and leaves no scars.
- Second degree A (superficial partial thickness) – affects almost the entire layer of the epidermis and superficial dermis. Wounds are usually vivid red, very painful, and are characterised by blisters. 2nd degree burn injury may leave slight discoloration, and sometimes scars.
- Second degree B (deep partial thickness) – the epidermis and deeper dermis layers are destroyed. In this type of injury superficial epidermal and skin necrosis is observed. This type of injury is very painful, blistering free, pale or pink, grey, brick red and even black. Moreover, they can leave negative hypertrophic scars.
- Third degree (full thickness) – extends through entire dermis. The wounds usually are pale brown, brown, pale yellow or red. They leave scars and can lead even to amputation.
- Fourth degree – extends through the entire skin, and into underlying fat, muscles, tendons, bones, joints.
Location
Burns occur in places of body contact with thermal factors.

Typically this affects:
- trunk
- upper limbs
- lower limbs
Where to seek help and advice
First degree burns
can be treated at home, and if there is in the progress in the treatment or complications appear consult your GP
Second and third degree burns
a hydrogel dressing should be applied as soon as possible, e.g. Medisorb G and immediately consult your doctor or contact the emergency station
Fourth degree burns
immediately contact the emergency station or the nearest hospital
Treatment
Depending on the burn degree the treatment is carried out in different ways.
First degree burns – affect only the epithelium. The place that was burned is red, slightly swollen and dry. The victim feels strong burning sensation. Quick application of a hydrogel dressing such Medisorb G allows for quick healing of the wound.
Second degree burns – damage the dermis. It becomes red, and on the surface there are blisters formed that fill with fluid tissue. Second degree burns are very painful. Similarly to the first degree burns rapid response using hydrogel dressings such Medisorb G allows for quick healing. If the burn is extensive, it requires hospitalisation.
Three and four degree burns – affect the tissue located under the skin. Also the connective tissue, blood vessels, muscles, and nerves can get damaged. The skin may take on waxy appearance, whitish or charred colour. The victim may not feel any pain because nerve endings have been destroyed. This type of burns require immediate medical help, sometimes even a skin graft or recovery in the hyperbaric chamber might be needed.
A common complication after recovering from burn wounds are hypertrophic scars and joint contractures. Their long recovery should be carried out using pressotherapy or rehabilitation of scars by means of compression products such as Codopress® combined with silicone dressings Codosil® ADHESIVE.
Prevention
Past statistics show that each year different types of burns affect about 1% of our population. According to these data, the number of Poles affected by various types of burns is up to 400 000 patients per year. Burns are very often associated with the type of activity of patients, as well as with age. Approximately 50-80% of burn victims are mainly children at the age 2 to 4 years.
Prevention of burns should primarily focus on the preparation of the house where the little man will feel safe:
- Never leave a young child alone.
- Avoid placing hot drinks, soups or dishes taken out directly from the oven on a table.
- In homes with young children – especially those crawling ones – there should be no tablecloths – pulling by the tablecloth a child pull down everything what stands on the table.
- Do not leave a turned on iron in the room, where a child is present; a turned off iron must cool down and also be out of reach of children.
- When cooking meals try to do use gas jets at the wall – those being away from your baby; you can use a special shield that prevents a child from touching a hot pot or pull it down.
- Owners of ceramic cooking plates should be aware that a turned off plate does not allow the child to notice the danger, and touching it before it cooled down can result in serious burns.
To sum up – parents should not leave their children unattended!